
Everyone Measures It But Us
The vital sign that predicts death better than cholesterol and why your cardiologist isn’t checking it.

Gary’s lipid panel is the kind most cardiologists dream to review with their patients. Total cholesterol in the 120s. Triglycerides under 60. HDL 51. LDL 61. ApoB 52. All well below the threshold where most of us even start a conversation about medication. By every conventional measure of cardiovascular risk, his circulation is excellent.
He was moderately athletic growing up, playing a variety of sports, was above average, and enjoyed them. But as a busy professional in his late forties, his athletic history has faded into the background. When I asked Gary about his daily activity, the clinical picture sharpened. As part of his emerging health journey, he’d recently purchased an Apple Watch. His average: about 5,200 steps per day. He used to jog two miles on the weekends, but with a six-year-old and a three-year-old, weekends had become stroller walks in the park, one to two miles at a casual pace. During the week, his step count often fell below 5,000. The weekends were pulling his daily step count average up.
Gary has a family history of coronary artery disease. His father and uncles developed coronary artery disease in their late sixties and early seventies. He and his wife had started their family a little later in life, beginning in their early forties. Now, at 48, with two young children counting on him, he was thinking differently about what it meant to be healthy. Gary didn’t want to just survive long enough to meet his grandchildren. He wanted to live well and be present for decades to come. Mobile, capable to hold, carry and play with his grandchildren. Gary had found and started reading the growing body of longevity and fitness writing and it led him to consult with me.
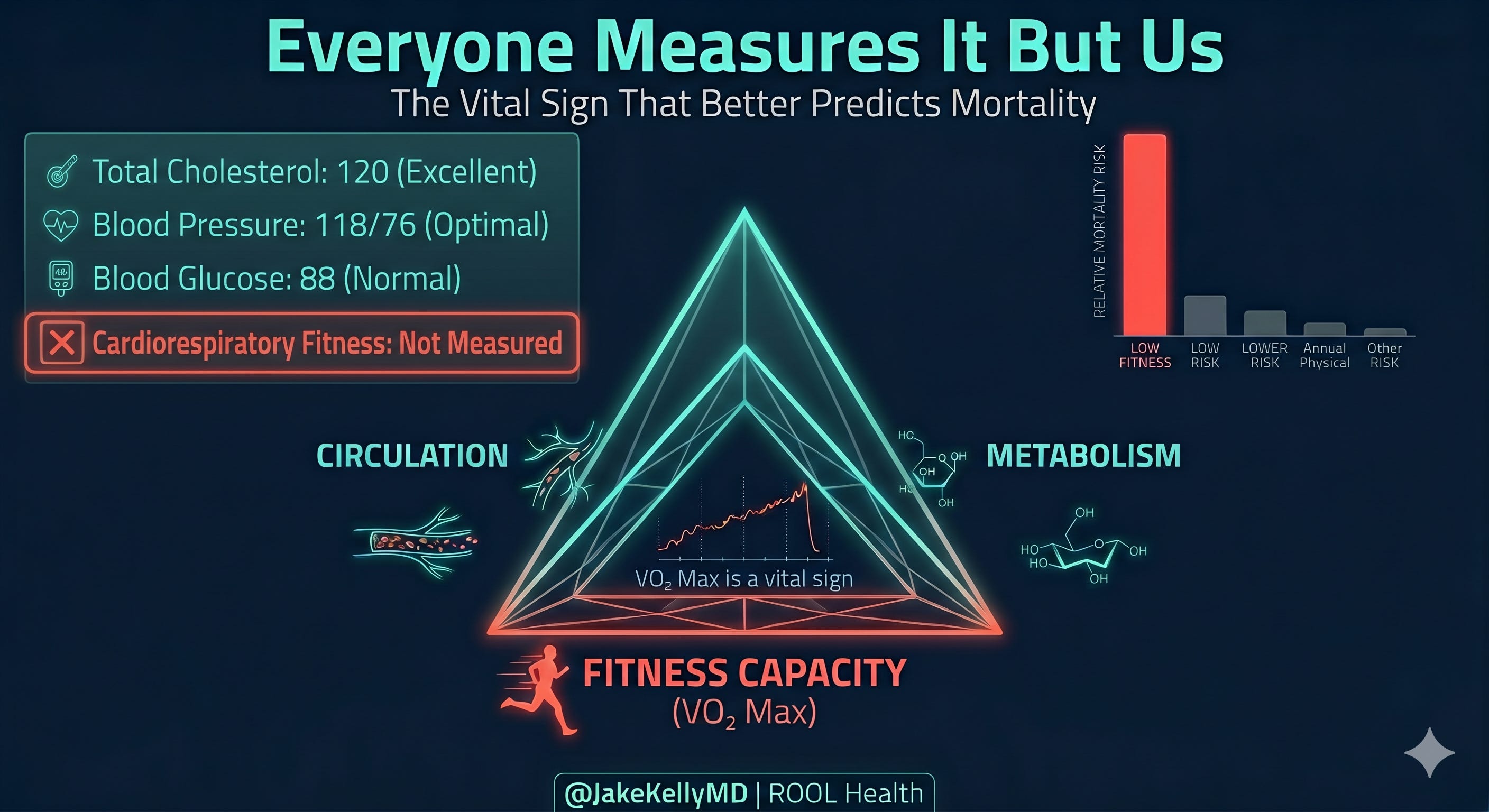
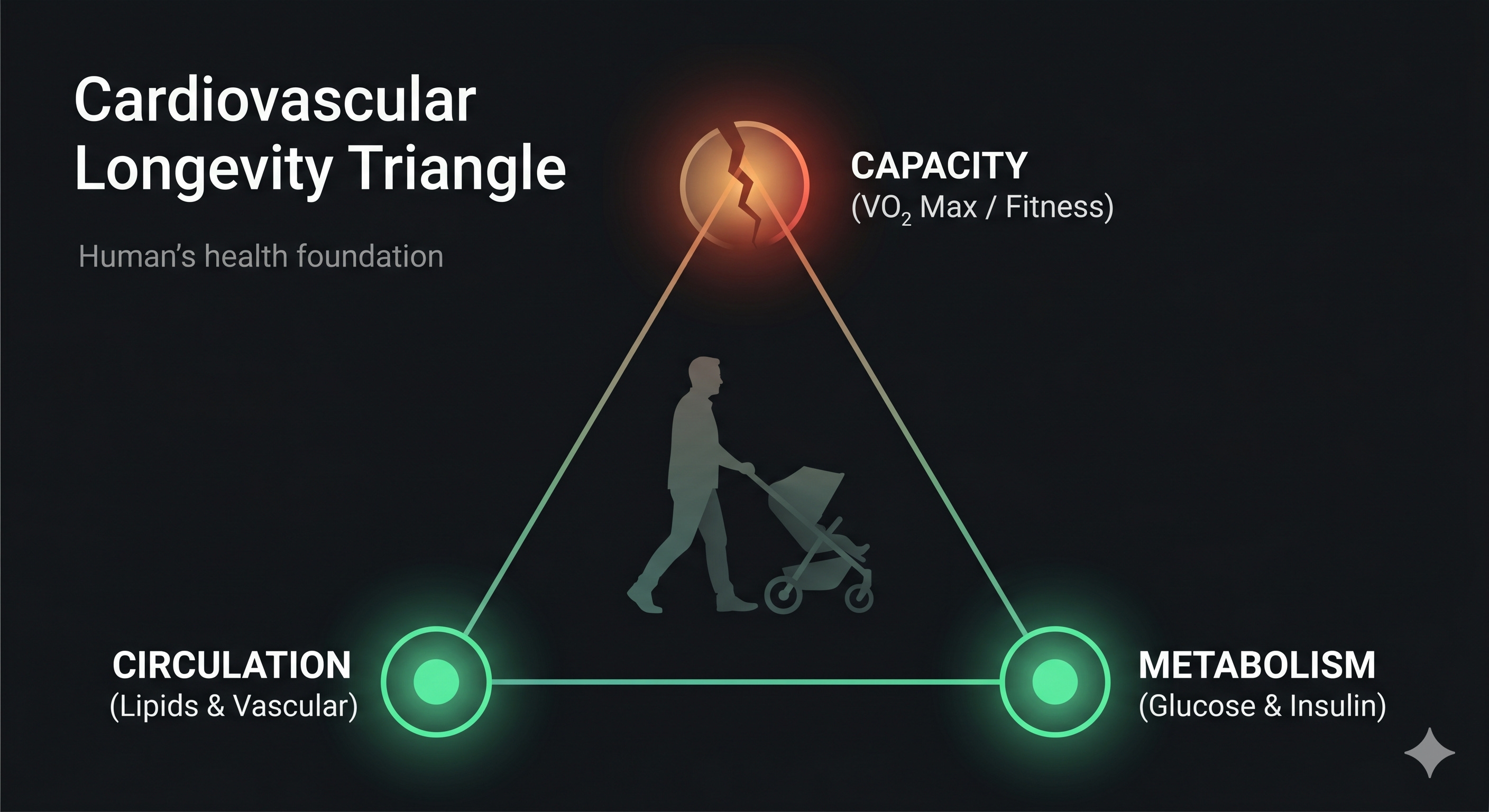
We talked through my framework, the Cardiovascular Longevity Triangle. Circulation, metabolism and cardiorespiratory fitness. Two of Gary’s three legs were outstanding. His lipids were enviable. His metabolic markers were clean. But the third leg, capacity, was unmeasured. I agreed to measure what he asked for: a cardiopulmonary exercise test.
His peak VO₂ came back at 31 ml/kg/min.
For a 48-year-old man, that places Gary between the 30th to 35th percentile according to the FRIEND registry, the national reference standard for directly measured cardiorespiratory fitness. Below the 50th percentile. Below average.
Gary’s lipid panel said he was fine. His fitness test said something else. One of the strongest predictors of whether my patients live or die isn’t on their lab panel. It’s a number most of them have never been told.
Gary decided to focus on the one leg of the Triangle that needed work. And that decision, not a medication, or a procedure, but a measurement followed by a plan, is the most important thing I did for him.
Here’s the problem: almost no one is doing what we did for Gary.
The data we keep ignoring
In 2009, Kodama and colleagues published a meta-analysis in JAMA of 33 studies spanning 102,980 healthy adults. The finding was simple and staggering: for every one-MET increase in cardiorespiratory fitness, all-cause mortality dropped 13 percent.
A MET, or metabolic equivalent of task, is a unit of energy expenditure. One MET equals the oxygen your body consumes at rest, about 3.5 ml of oxygen per kilogram of body weight per minute. Sitting quietly is 1 MET. A slow walk is about 2. A brisk walk is 3 to 4. Jogging is 7 to 8. Running hard is 10 METs or above. When we say someone achieved “9 METs” on a treadmill test, it means their body was consuming nine times the oxygen it uses at rest.
So one MET higher. That’s the difference between a slow walk and a brisk walk. A 13 percent reduction in dying.
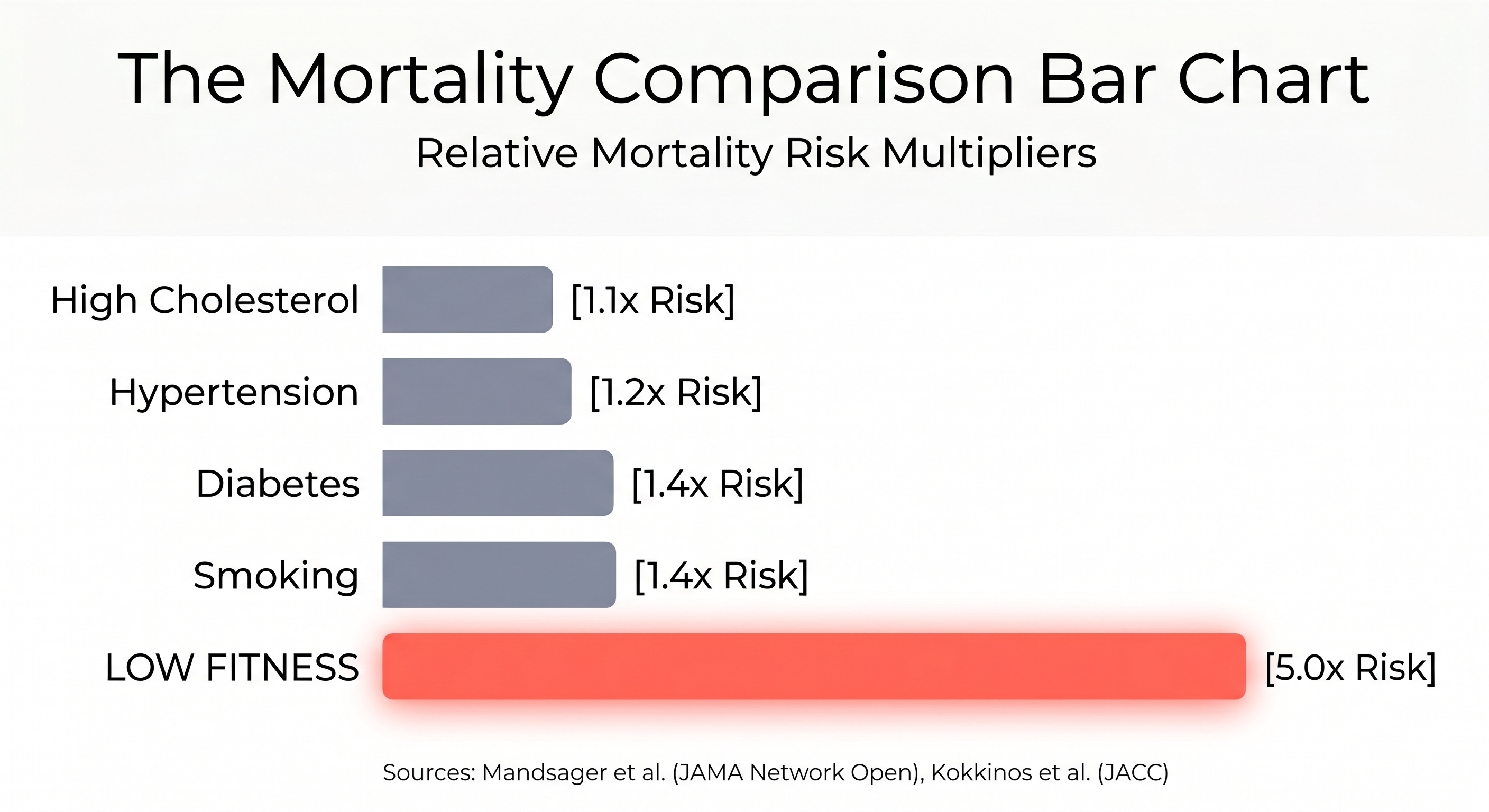
In 2018, Mandsager and colleagues at the Cleveland Clinic published exercise treadmill data on 122,007 consecutive patients in JAMA Network Open. They stratified patients from low fitness to elite fitness and measured long-term mortality. The result: a five-fold difference in death between the least fit and the most fit. Being unfit carried the same mortality risk as smoking. And diabetes.
Your patient who can’t walk briskly up a hill carries the same mortality risk as the one who still smokes a pack a day.
In 2022, Kokkinos and colleagues extended this to 750,302 US veterans, published in JACC. The conclusion was even more direct: low cardiorespiratory fitness was a stronger predictor of death than any single traditional cardiac risk factor. More than hypertension. Diabetes. Coronary artery disease. And there was no upper limit of benefit. The fittest patients lived the longest. Period.
By 2024, Lang and colleagues synthesized the entire field: 20.9 million observations across 199 cohorts, published in the British Journal of Sports Medicine. High fitness versus low fitness: 53% lower all-cause mortality. For heart failure incidence specifically: 69% lower.
It’s not just your baseline. Kokkinos showed in a 2023 follow-up study of 93,060 veterans with serial exercise testing that each one-MET improvement over time was associated with a 15 percent reduction in mortality. The number moves and the trajectory matters.
The American Heart Association recognized all of this in 2016, publishing a scientific statement in Circulation titled, “Importance of Assessing Cardiorespiratory Fitness in Clinical Practice: A Case for Fitness as a Clinical Vital Sign.” They called CRF a vital sign, in those exact words, and recommended it be assessed routinely in all healthcare settings.
That was ten years ago.
Almost nothing has changed.
So who actually measures it?
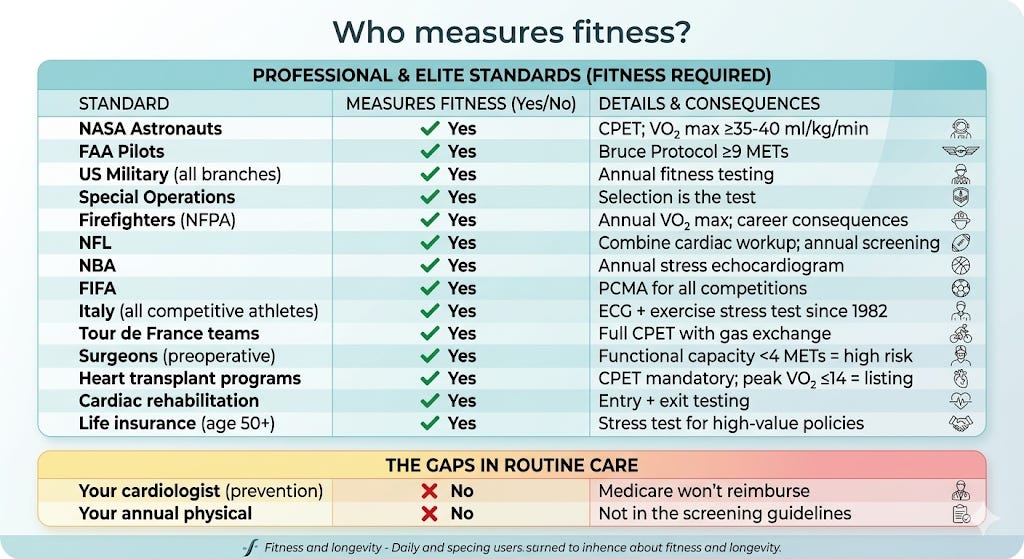
I started making a list of every institution, organization and profession that formally measures cardiorespiratory fitness. It got long.
NASA measures VO₂ max on every astronaut with a metabolic cart, the gold standard, before flight, monthly during spaceflight, and after return. The requirement: at least ~ 35 ml/kg/min for space station missions. At least 40 for Mars. If the number drops, the mission changes.
The FAA requires every pilot flagged with a cardiac condition to complete the Bruce Protocol treadmill test. Minimum: Stage III, at least nine minutes, approximately nine METs, 100% of predicted maximum heart rate. Fail and you don’t fly.
Every branch of the US military tests aerobic fitness annually. The Army’s ACFT includes a two-mile run, a direct proxy for cardiorespiratory fitness. Research shows that VO₂ max explains 38 percent of the variance in total ACFT scores. For Special Operations forces, including Navy SEALs, Army Rangers, British SAS, German KSK, and Israeli Sayeret Matkal, selection itself is a cardiorespiratory fitness test. You either have the aerobic capacity or you’re out.
Fire departments have what may be the most consequential standard of all. For decades, the National Fire Protection Association mandated a flat, absolute aerobic floor of 12 METs (42 ml/kg/min) for all personnel. But in a massive shift to align with modern clinical data, the updated standard (NFPA 1580) now utilizes strict, age- and sex-adjusted population percentiles. Fall below the 35th percentile and you are restricted from essential firefighting duties. Land between the 35th and 50th percentile and you are placed on a mandatory, career-altering cardiorespiratory exercise program. These aren't suggestions. They are operational standards.
Why? Because cardiac arrest is the number one killer of firefighters in the line of duty. They started measuring fitness because their people were dying.
The NFL Combine runs an intensive cardiac workup on every prospective player: ECG, echocardiogram, stress testing when warranted. Two to three players are red-flagged every year. The NBA goes further: mandatory annual ECG and stress echocardiogram for every active player. Not triggered by symptoms. Not conditional. Mandatory. Administered in partnership with Columbia University, results stored in a centralized database. Basketball has a higher rate of sudden cardiac death than other professional sports. So they measure.
FIFA requires a Pre-Competition Medical Assessment for all international competitions, mandatory since 2006, with ECG plus additional testing when indicated. Italy stands alone globally. Since 1982, Italian law has mandated both a resting ECG and an exercise stress test for every competitive athlete at every level. Not just professionals. All of them. And the data suggests it’s working. Italy has documented a reduction in sudden cardiac death from hypertrophic cardiomyopathy since implementing the program.
Tour de France cycling teams perform full cardiopulmonary exercise testing with gas exchange analysis, including VO₂ max, lactate thresholds and ventilatory efficiency, on every rider. These are the most physiologically measured humans on earth.
Surgeons have their own version. Before major noncardiac surgery, functional capacity is assessed, formally or informally. Can the patient climb two flights of stairs without stopping? That’s roughly four METs. Below four METs, surgical risk increases substantially. Increasingly, CPET is used for formal preoperative risk stratification: an anaerobic threshold below 9 to 11 ml/kg/min predicts ICU admission and mortality.
Life insurance companies require a treadmill stress test for applicants over 50 seeking high-value policies. They’re pricing your survival. They want the number.
Cardiac rehabilitation programs test exercise capacity at entry and at exit. The AHA and AACVPR set a goal of at least 15 percent improvement in peak VO₂ over the course of rehabilitation.
In heart failure, CPET isn’t optional. It’s mandatory. In 1991, Mancini and colleagues published the landmark study in Circulation establishing that peak VO₂ at or below 14 ml/kg/min identifies patients who benefit from heart transplantation. In 1995, Lynne Warner Stevenson refined the approach in a study of 737 consecutive advanced heart failure patients in JACC, showing that peak VO₂ should be measured on optimal medical therapy and that an improvement of at least 2 ml/kg/min predicted better survival, sometimes enough to defer transplant entirely. Today, the ISHLT guidelines make maximal CPET a Class I recommendation for transplant evaluation.
In advanced heart failure, this test decides whether you live or die.
The gap
And then there’s the 55-year-old sitting in my prevention clinic.
Family history of heart disease. Desk job. Resting heart rate of 78. Lipid panel looks adequate. Blood pressure is controlled. The standard risk calculator puts him at intermediate risk.
Nobody has measured his fitness. Nobody has even asked.
I could estimate his cardiorespiratory fitness in 30 seconds using the Duke Activity Status Index, a simple set of questions about exercise tolerance. I could get a rough MET estimate from his age, weight, resting heart rate and activity level using a validated nonexercise equation. I could refer him for a treadmill test or a full CPET.
But Medicare will not reimburse an exercise stress test for an asymptomatic patient. The CPT codes exist, 93015 through 93018 and they’re used every day for chest pain evaluation, post-revascularization monitoring, arrhythmia assessment, valvular disease management, preoperative clearance and transplant candidacy. The test exists. The infrastructure exists. Cardiologists know how to order it, read it and act on it.
The exclusion is specific: asymptomatic screening. The one population where the mortality data is strongest.
The AHA called cardiorespiratory fitness a clinical vital sign. The ACC/AHA ASCVD risk calculator does not include it. The USPSTF has actually downgraded exercise stress testing in low-risk asymptomatic adults. The field that identified the relationship between fitness and mortality has not built a system to measure fitness in the people most at risk of dying.
We measure cholesterol. We measure blood pressure. We measure glucose, hemoglobin A1c, BMI and resting heart rate. We do not routinely measure the single variable that predicts death better than all of them.
What you can do about it
The metric debate, VO₂ max versus peak METs versus wearable estimates, is real and I’ll address it along with my personal thoughts in detail in a future post. Topol is right that 99 percent of the mortality data comes from estimated peak METs on treadmill tests, not from gas-exchange VO₂ max. Attia is right that the signal is powerful regardless of how you label it. But the argument about which metric to use has become a distraction from the more important question: are you (we?) measuring it at all?
Here’s what I want you to take from this.
If you’re a patient: Ask your doctor a simple question at your next visit: what is my estimated cardiorespiratory fitness? If they’ve never assessed it, that’s a gap worth closing. Know the threshold: the Kodama data shows that 7.9 METs is an inflection point for mortality. Can you walk briskly up two flights of stairs without stopping? That’s roughly four METs. Can you jog for ten minutes? Roughly seven to eight. If you wear a Garmin or Apple Watch, use the VO₂ max estimate for trend, not for the absolute number. If it’s declining over six months, pay attention. Your trajectory matters more than any single reading.
If you’re a clinician: Start estimating CRF at every visit. It takes 30 seconds. A simple question about exercise tolerance gives you a MET estimate that predicts your patient’s survival better than their lipid panel. The AHA called this a clinical vital sign a decade ago. We owe our patients at least an estimate.
If you’re in the fitness community: The debate between Topol, Attia and Magness about whether we’ve created a counterproductive “VO₂ max craze” is interesting. But don’t miss the forest. The data across 20.9 million observations says the same thing: raise your fitness and you lower your risk of dying. The UK Biobank data from Kim and colleagues shows that cardiorespiratory fitness plus grip strength together reduces mortality more than either alone. Train both.
The strongest predictor of survival we have is free to estimate, inexpensive to measure and modifiable at any age. After nine months of endurance training, adults in their sixties increased their VO₂ max by 19 to 22 percent. An 80-year-old man holds a recorded VO₂ max of 50 ml/kg/min, equivalent to an inactive 25-year-old. The number moves.
We just have to start measuring it.
If you know someone whose doctor has never asked about their fitness level, send them this.
If this changed how you think about cardiorespiratory fitness and survival, share it with someone who needs to hear that the strongest predictor of longevity isn’t on their lab panel.
For individuals who want this integrated approach, where cardiorespiratory fitness, circulation, and metabolic health are treated as a single system: jakekellymd.com.
Jake Kelly, MD, MHS, FACC is a board-certified performance and preventive cardiologist, Wasserman-certified in cardiopulmonary exercise testing, ACC Governor for Alaska and founder of ROOL Health, a cardiometabolic longevity practice in Anchorage.
Legal Medical Disclaimer
The information provided on this site including articles, newsletters, social-media posts, videos, and downloadable resources is intended for general educational purposes only and does not constitute medical advice, diagnosis, or treatment. Your use of this content does not establish a physician–patient relationship with me or any contributor. Always seek the guidance of your own physician or another qualified health-care provider before beginning an exercise program, undergoing diagnostic testing, making lifestyle changes, or starting or stopping any medication or supplement. Never disregard professional medical advice or delay seeking care because of something you have read here. If you think you may have a medical emergency, call 911 (or your local emergency service) immediately.
References
Ross R, Blair SN, Arena R, et al. Importance of assessing cardiorespiratory fitness in clinical practice: a case for fitness as a clinical vital sign: a scientific statement from the American Heart Association. Circulation. 2016;134(24):e653-e699.
Ross R, Arena R, Myers J, Kokkinos P, Kaminsky LA. Update to the 2016 American Heart Association cardiorespiratory fitness statement. Prog Cardiovasc Dis. 2024;83:10-15.
Kodama S, Saito K, Tanaka S, et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: a meta-analysis. JAMA. 2009;301(19):2024-2035.
Mandsager K, Harb S, Cremer P, et al. Association of cardiorespiratory fitness with long-term mortality among adults undergoing exercise treadmill testing. JAMA Netw Open. 2018;1(6):e183605.
Kokkinos P, Faselis C, Samuel IBH, et al. Cardiorespiratory fitness and mortality risk across the spectra of age, race, and sex. J Am Coll Cardiol. 2022;80(6):598-609.
Kokkinos P, Faselis C, Samuel IBH, et al. Changes in cardiorespiratory fitness and survival in patients with or without cardiovascular disease. J Am Coll Cardiol. 2023;81(12):1137-1147.
Lang JJ, Prince SA, Merucci K, et al. Cardiorespiratory fitness is a strong and consistent predictor of morbidity and mortality among adults: an overview of meta-analyses representing over 20.9 million observations from 199 unique cohort studies. Br J Sports Med. 2024;58(10):556-566.
Mancini DM, Eisen H, Kussmaul W, Mull R, Edmunds LH Jr, Wilson JR. Value of peak exercise oxygen consumption for optimal timing of cardiac transplantation in ambulatory patients with heart failure. Circulation. 1991;83(3):778-786.
Stevenson LW, Stevenson WG, Middlekauff HR, et al. Improving survival for patients with advanced heart failure: a study of 737 consecutive patients. J Am Coll Cardiol. 1995;26(6):1417-1423.
Heidenreich PA, Bozkurt B, Aguilar D, et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2022;79(17):e263-e421.
Kaminsky LA, Imboden MT, Arena R, Myers J. Reference standards for cardiorespiratory fitness measured with cardiopulmonary exercise testing using cycle ergometry: data from the Fitness Registry and the Importance of Exercise National Database (FRIEND) Registry. Mayo Clin Proc. 2017;92(2):228-233.
Topol E. The flawed VO₂ max craze. Ground Truths (Substack). February 23, 2026.
Kim Y, White T, Wijndaele K, et al. The combination of cardiorespiratory fitness and muscle strength, and mortality risk. Eur J Epidemiol. 2018;33(10):953-964.
Great article!
We
Must
Move!
Education is the answer. More Health and Physical Education in schools - every day for every student... and yet school curriculum is going in the opposite direction. I am routinely shocked when I hear "educated" professionals say something that reveals they have little understanding of how our bodies function. Your articles are so informative. When will you write your Book of Everyday Health for us?