
Rx: Sleep
Dose 7–8 hours. Frequency nightly. Refills ∞.

Joan came in this week for a murmur evaluation. She was doing well: exercising, eating thoughtfully, in a strong marriage. As we were wrapping up the visit, I asked the question I ask every patient: how is your sleep?
Her answer: terrible.
This is what I hear frequently from seemingly dialed in patients. Patients have thoughtful health forward plans on diet, exercise and all the visible aspects of their lie. Sleep is where the truth comes out and it is the part of health maintenance that I am coming to care most about, because sleep sits upstream of nearly everything I treat: metabolic, cardiorespiratory fitness, circulation and cognitive health.
I told Joan about the two questions I ask myself every morning:
Did I have a good night’s sleep?
How do I make sure tonight is as good, or better?
This is my sleep framework. Last night’s sleep is the only outcome that matters. Tonight is the only thing you can change. And the answer to question #2 almost never happens at bedtime. It happens hours earlier, in the choices most people don’t realize they’re making throughout their daily lives.
We walked through her pattern. She was disciplined on caffeine: none after lunch. But she was eating right up to bedtime and scrolling on her phone in bed. Two simple adjustments. No medication, no supplements. This is where most patients are losing ground on good (better?) sleep.
I’ve written about sleep before. This is what I’d say now.
Rx: Sleep Dose: 7–8 hours Frequency: Nightly Refills: Unlimited Expiration: None
I write that on a real prescription pad. Every patient gets one. I do it because the data on sleep, 2024 through 2026, has become so strong it feels like malpractice not to take it seriously. The AHA elevated sleep into Life’s Essential 8 in 2022, then released two more scientific statements (2024), 2025 on cardiometabolic health explicitly recognizing not just sleep duration but sleep regularity as independent predictors of disease and death. The FDA approved tirzepatide for obstructive sleep apnea last year. The 2026 ADA Standards of Care now name short sleep as a modifiable risk factor for type 2 diabetes.
Sleep is the most underprescribed intervention in medicine. Let’s fix that.
I Call Sleep a Religious Experience
I mean it. The condition. The ritual. The reverence.
You wouldn’t expect to perform surgery in a noisy room with the lights on and your phone buzzing. You shouldn’t expect to perform sleep that way either. Mood, setting and pattern do most of the work towards improving and having good sleep. The drug part, the actual physiology, only kicks in when you’ve built the runway.
The 6+ / 3 / 2 / 1 Sleep Runway
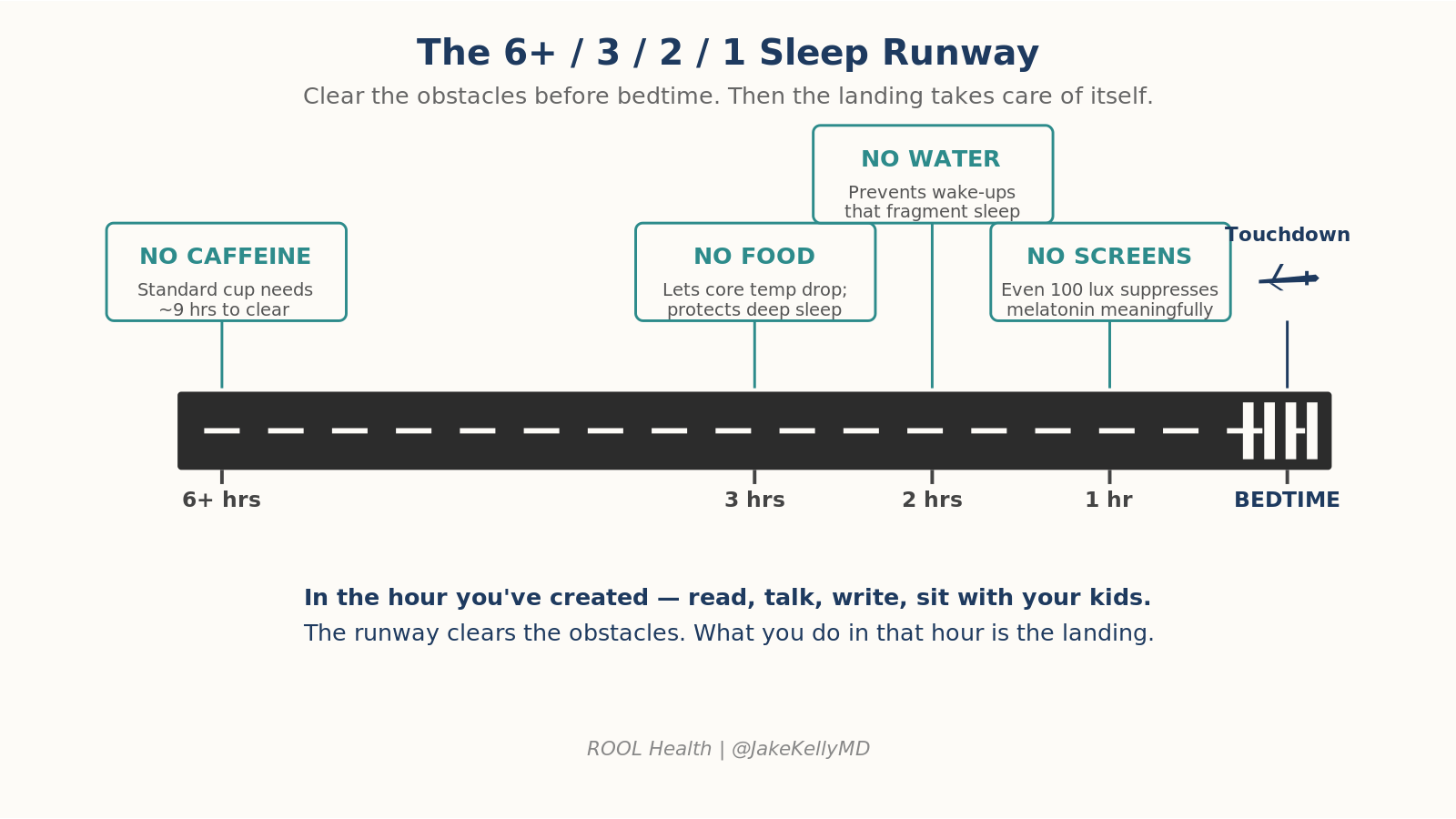
Most of what people get wrong about sleep happens in the hours before they get into bed. Think of bedtime like landing a plane. You don’t pull the nose up at the last second. You set up a runway.
6+ hours before bed: No caffeine. This is the rule I get the most pushback on. The pharmacology is unforgiving. Caffeine’s half-life in adults averages 2.5–4.5 hours, but a 2023 dose-response meta-analysis showed that a standard cup of coffee (~107 mg) needs about 8.8 hours before bed to avoid measurable reductions in total sleep time. A 200 mg pre-workout? Closer to 13 hours. CYP1A2 genetics, oral contraceptives and smoking status shift the pharmacodynamics further back. A 2 p.m. coffee for a 10 p.m. bedtime is reducing your evening sleep quality.
3 hours before bed: No food. Eating late raises core body temperature exactly when it needs to drop, blunts melatonin onset and forces the gut into digestion when the body should be entering recovery mode. Joan was eating dinner past 8. We moved it earlier. The cleaner the runway, the easier and deeper we move into slow-wave sleep.
2 hours before bed: No water. The bladder doesn’t care how tired you are. Each nocturnal wake-up fragments sleep architecture and fragmentation, not just total sleep time, is what predicts cognitive decline and amyloid deposition.
1 hour before bed: No screens. Partly about blue light (even ~100 lux of typical indoor lighting can meaningfully suppress melatonin) and partly about content. The phone is not neutral. Doomscrolling spikes cortisol. News, email and social media delay sleep onset in ways that aren’t fully explained by light alone.
That last hour is not empty space. It’s where you read, talk to your partner, stretch, sit with your kids or write. The runway clears the obstacles. What you do in the hour is the landing.
The Other Half: Building Sleep Pressure During the Day
I saw a different patient earlier this week with a more significant sleep problem. We didn’t change much about her evening routine. We changed her day.
Most people think about sleep as a 60-minute project that starts at 10 p.m. It isn’t. Sleep is a 16-hour project that starts the moment you wake up.
Here’s why: adenosine, the molecule that makes you sleepy, accumulates in your brain every hour you’re awake. That accumulation is the engine of sleep. If you nap too long, sit in dim light all day, or stay sedentary, you don’t build enough pressure for sleep to come easily. You arrive at bedtime with an empty tank, then wonder why you can’t sleep.
This is the part that’s fascinated me more as I’ve aged: sleep is something you work for throughout the day and it’s also something that benefits you throughout the day. The work and the reward are the same thing. The investment is the return.
The day-side of the protocol:
Morning light within an hour of waking. 10–30 minutes outside, no sunglasses if you can manage it. This sets your circadian clock and starts the adenosine engine.
Move. Walking, training, anything that gets your nervous system out of low-power mode. Movement is fuel for sleep.
Skip the long afternoon nap. Keep naps under 20 minutes if you nap at all. Longer naps blow off your sleep pressure.
Front-load your eating window. Time-restricted eating that closes by 7 p.m. supports both metabolism and sleep.
How Sleep Actually Works
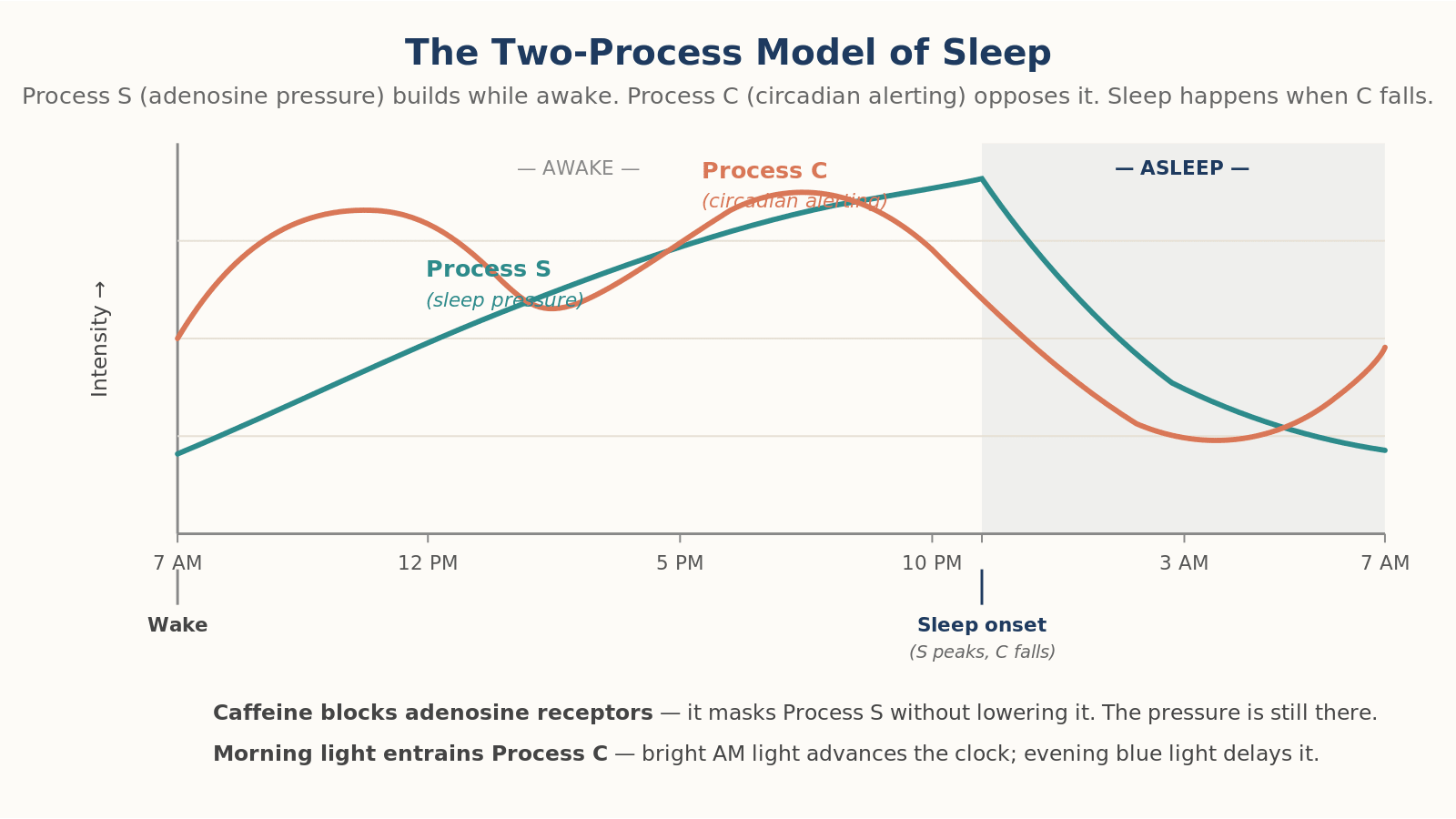
Sleep isn’t passive. Two systems govern it.
Process C (Circadian). Your suprachiasmatic nucleus runs a roughly 24-hour clock that controls alertness, body temperature and hormone release. It’s calibrated by light. Morning bright light advances the clock; evening blue light delays it. The 2022 international consensus on indoor light now uses melanopic equivalent daylight illuminance (melanopic EDI) as the standard. The practical translation hasn’t changed: get bright light in your eyes within an hour of waking, dim the lights after sunset.
Process S (Sleep pressure). Adenosine builds while you’re awake. Sleep clears it. Caffeine blocks adenosine receptors. It doesn’t reduce the pressure, it masks it. When caffeine wears off, the accumulated adenosine is still there waiting.
Inside that 7- to 8-hour window, you cycle through stages every ~90 minutes:
N1, N2: Light sleep, transition phases.
N3 (slow-wave / deep sleep): Front-loaded in the first half of the night. Where the immune system primes, growth hormone releases, tissue repairs, and, critically, the glymphatic system clears amyloid-β and tau from the brain. The 2024 AHA scientific statement on sleep and brain health placed glymphatic clearance at the center of dementia prevention.
REM: Back-loaded toward morning. Memory consolidation, emotional processing.
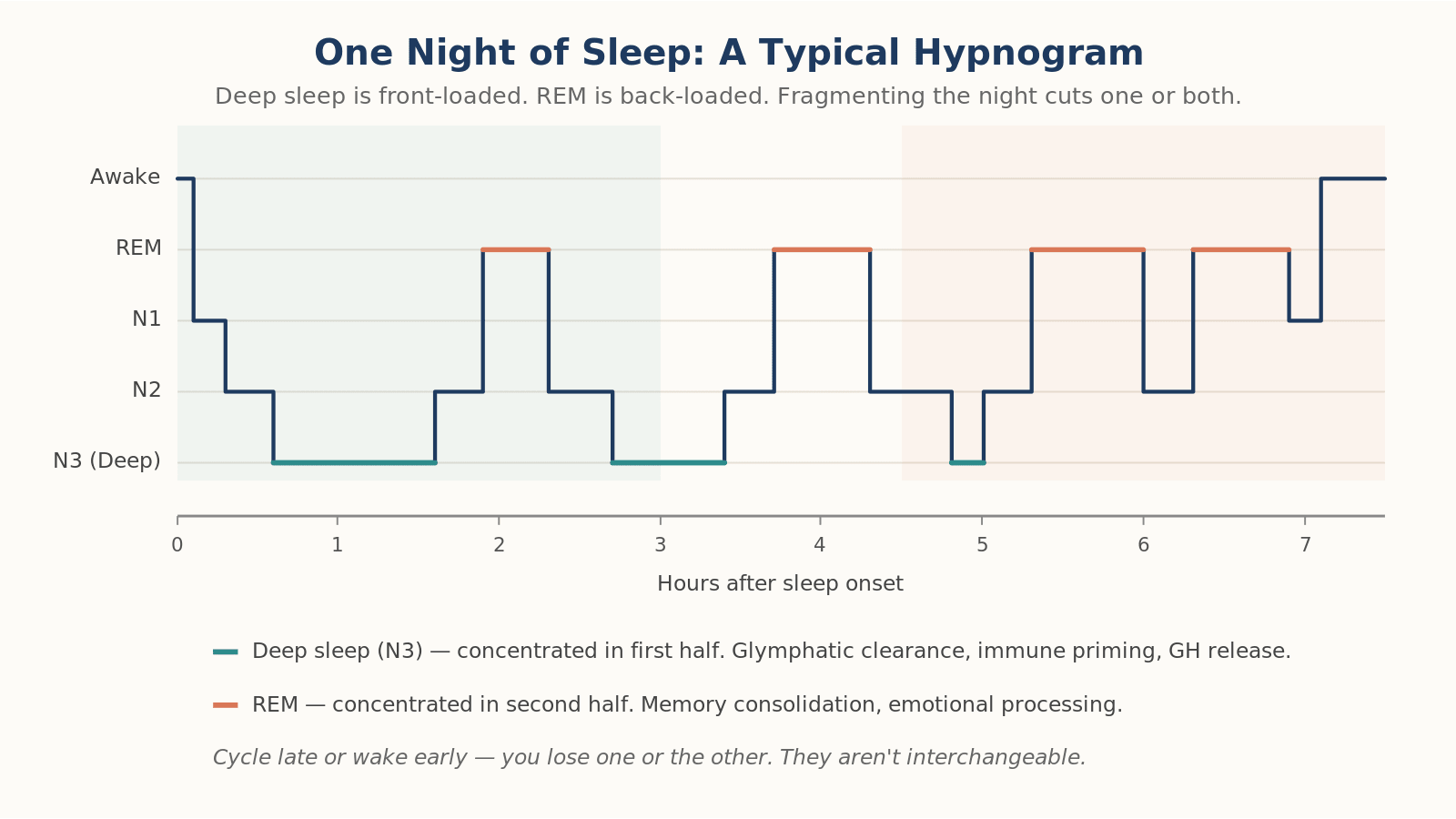
Cut the night short by going to bed late and you preferentially lose REM. Wake at 4 a.m. and can’t get back to sleep and you lose the deep sleep cycles you haven’t completed. Both are important. Neither is replaceable.
The Evidence
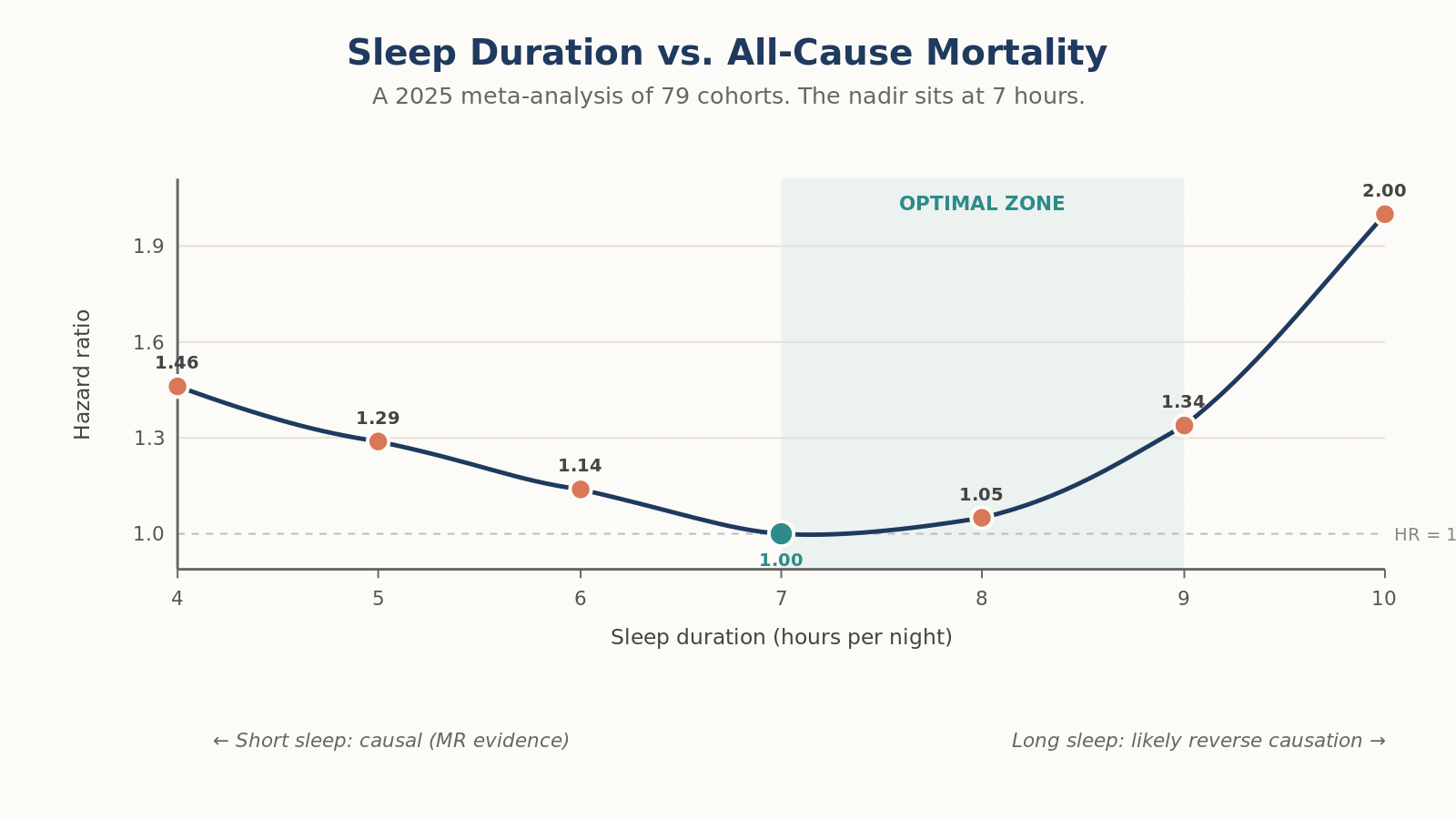
Mortality. A 2025 meta-analysis of 79 cohort studies confirmed the U-shape: short sleep (<7 hours) carries a 14% higher all-cause mortality risk; long sleep (≥9 hours) carries 34% higher risk, more pronounced in women. UK Biobank accelerometry (n = 88,282), using objective measurement rather than self-report, found a 29% higher mortality risk at 5 hours per night. Mendelian randomization suggests the short-sleep association is causal; the long-sleep association is likely confounded by underlying illness.
Cardiovascular disease. Objectively measured sleep under 7 hours raises the risk of incident CVD, MI, heart failure, and atrial fibrillation, with a dose-response curve that steepens below 7 hours. Genetic studies confirm short sleep causes hypertension and coronary artery disease. It isn’t just correlated with them.
Dementia. Insomnia is associated with a 53% increase in dementia risk. Both short and long sleep duration have been linked to at least a doubling of risk. Without adequate deep sleep, the glymphatic system fails to clear the amyloid and tau that, over decades, become Alzheimer’s pathology. A 2024 JAMA Neurology study showed disrupted 24-hour activity rhythms predicted subsequent amyloid-β deposition, especially in APOE4 carriers.
Metabolism. A 2024 randomized crossover trial in women found that just six weeks of 1.5 hours less sleep per night raised fasting insulin and HOMA-IR without any change in body weight. The 2026 ADA Standards of Care now formally recognize sleep duration as a modifiable risk factor for type 2 diabetes, with up to 50% increased risk at the extremes.
The New Story: Sleep Regularity
This is the finding I want every patient to hear. The 2024 Windred et al. UK Biobank study (n = 60,977, >10 million hours of wrist-worn accelerometry) showed that how consistent your sleep timing is may predict mortality better than how long you sleep.
People in the top quintile of sleep regularity had 20–48% lower all-cause mortality, 16–39% lower cancer mortality, and 22–57% lower cardiometabolic mortality compared to the most irregular quintile. Adding sleep duration to a regularity-based model didn’t significantly improve prediction. The 5th percentile of regularity carried a 53% higher mortality risk than the median.
The 2025 AHA scientific statement on multidimensional sleep health now lists regularity as a distinct sleep dimension with independent cardiometabolic implications.
The practical message: going to bed at midnight every night may beat the pattern of 10 p.m. some nights and 2 a.m. others, even if the average is the same. Shift workers and college students living through “social jet lag” should hear this loudly. So should anyone whose weekend schedule looks nothing like their weekday one.
The body wants rhythm. Cadence is medicine.
Wearables: What They Get Right, What They Don’t
A 2025 meta-analysis of 24 validation studies found that consumer wrist-worn devices systematically overestimate total sleep time by about 17 minutes and underestimate wake-after-sleep-onset by about 13 minutes. Sleep/wake detection is reasonably accurate (>95% sensitivity for sleep). Sleep stage classification still isn’t.
Wearables validated against polysomnography in head-to-head 2024 data:
Oura Ring Gen3: Best overall stage agreement; no significant difference from PSG for any sleep stage duration.
WHOOP: Comparable multi-state agreement to Oura.
Apple Watch Series 8: High REM sensitivity but underestimates deep sleep by ~43 minutes.
What to track: weekly average total sleep time, bedtime and wake-time consistency (your SRI proxy), resting heart rate trends. What to mostly ignore: night-to-night REM and deep sleep percentages.
Sleep Apnea: The Tirzepatide Era
If you snore, wake unrefreshed, have a thick neck or morning headaches, or your partner has watched you stop breathing, get evaluated. The STOP-BANG questionnaire is the most sensitive primary care screen.
The biggest change in the OSA landscape: tirzepatide is now FDA-approved for moderate-to-severe OSA in adults with obesity. In the SURMOUNT-OSA trials, it reduced the apnea-hypopnea index by 50–59%, and 42–50% of patients reached levels where CPAP would no longer be indicated. CPAP remains first-line for respiratory control, but a 2025 review supports a combined airway-metabolic approach: CPAP for the airway, GLP-1 for the underlying obesity that drives it.
When the Runway Doesn’t Work: CBT-I
For chronic insomnia, the first-line treatment is not a sleeping pill. It’s cognitive behavioral therapy for insomnia (CBT-I). A 2024 network meta-analysis confirmed CBT-I produces better long-term remission than pharmacotherapy. About 50% of patients reach remission after 6–8 weeks; 40–45% sustain it at one year.
Digital CBT-I (Sleepio, SHUTi, Somryst) has matured into a real option, with effect sizes comparable to in-person therapy and outperforming medication in head-to-head comparisons. If you’ve been on Ambien or trazodone for years, ask your physician about CBT-I.
The Playbook
Ask the morning questions. Did I sleep well? How do I make tonight better?
Build pressure during the day. Morning light. Movement. Skip the long nap.
Run the 6+ / 3 / 2 / 1 runway.
Sleep regularity matters as much as duration. Same bedtime, same wake time, weekends included.
Cool the cave. 64–68 °F.
Move your caffeine cutoff to noon. Earlier if you’re a slow metabolizer.
Screen for OSA if you snore. STOP-BANG → sleep study → treatment.
CBT-I before pills for chronic insomnia.
Joan left with a sleep prescription. Two adjustments: dinner earlier, phone out of the bedroom. That’s where most of the work happens. The runway, not the bed.
Sleep is something you work for throughout the day. It is also something that benefits you throughout the day. The work and the reward are the same thing. That’s why I treat it as a religious experience, and why I write it on a real prescription pad. Same seriousness as a statin. Larger upside.
Seven to eight hours. Same time, every night. The most underprescribed intervention in medicine.
References
Ungvari Z, et al. Imbalanced sleep increases mortality risk by 14–34%: a meta-analysis. GeroScience. 2025.
Saint-Maurice PF, et al. Associations between actigraphy-measured sleep duration, continuity, and timing with mortality in the UK Biobank. Sleep. 2024.
Ai S, et al. Causal associations of short and long sleep durations with 12 cardiovascular diseases: linear and nonlinear Mendelian randomization analyses in UK Biobank. Eur Heart J. 2021.
Windred DP, et al. Sleep regularity is a stronger predictor of mortality risk than sleep duration: a prospective cohort study. Sleep. 2024.
Gottesman RF, et al. Impact of sleep disorders and disturbed sleep on brain health: a scientific statement from the American Heart Association. Stroke. 2024.
St-Onge MP, et al. Multidimensional sleep health: definitions and implications for cardiometabolic health. Circ Cardiovasc Qual Outcomes. 2025.
Zuraikat FM, et al. Chronic insufficient sleep in women impairs insulin sensitivity independent of adiposity changes. Diabetes Care. 2024.
American Diabetes Association. Standards of Care in Diabetes, 2026. Diabetes Care. 2026.
Malhotra A, et al. Tirzepatide for the treatment of obstructive sleep apnea and obesity. NEJM. 2024.
Gardiner C, et al. The effect of caffeine on subsequent sleep: a systematic review and meta-analysis. Sleep Med Rev. 2023.
Morin CM, Buysse DJ. Management of insomnia. NEJM. 2024.
Lee YJ, et al. Performance of consumer wrist-worn sleep tracking devices compared to polysomnography: a meta-analysis. J Clin Sleep Med. 2025.
Brown TM, et al. Recommendations for daytime, evening, and nighttime indoor light exposure to best support physiology, sleep, and wakefulness in healthy adults. PLoS Biol. 2022.
Lastra AC, et al. Diagnosis and treatment of obstructive sleep apnea. JAMA Intern Med. 2025.
Nguyen Ho PT, et al. Sleep, 24-hour activity rhythms, and subsequent amyloid-β pathology. JAMA Neurol. 2024.
Lloyd-Jones DM, et al. Life’s Essential 8: updating and enhancing the American Heart Association’s construct of cardiovascular health. Circulation. 2022.
Robbins R, et al. Accuracy of three commercial wearable devices for sleep tracking in healthy adults. Sensors. 2024.
Patient names and identifying details have been changed to protect privacy.
If you found this article valuable, share it with someone whose sleep could be better.
For patients who want this kind of thinking applied to their own cardiovascular health, longevity and performance, visit jakekellymd.com.
Jake Kelly, MD, MHS, FACC is a board-certified performance and preventive cardiologist, ACC Governor for Alaska and founder of ROOL Health, a cardiometabolic longevity practice in Anchorage.
Legal Medical Disclaimer
The information provided on this site including articles, newsletters, social-media posts, videos, and downloadable resources is intended for general educational purposes only and does not constitute medical advice, diagnosis, or treatment. Your use of this content does not establish a physician–patient relationship with me or any contributor. Always seek the guidance of your own physician or another qualified health-care provider before beginning an exercise program, undergoing diagnostic testing, making lifestyle changes, or starting or stopping any medication or supplement. Never disregard professional medical advice or delay seeking care because of something you have read here. If you think you may have a medical emergency, call 911 (or your local emergency service) immediately.
Helpful information about the importance of regular sleep schedule. I certainly learned this when my children were babies and as they grew up. Sleep schedule interruptions = cranky kids. Somehow we learn to disguise this problem from our adult selves as we push through busy higher education and career life.
In my early 40s, I began to have a harder time falling asleep, especially on Sunday nights......hmmm.... Then I read somewhere that said we should get up at the same time every day, no matter how late we stayed up socializing.
As soon as I started getting up at the same time on weekend mornings that I did on work days, the Sunday night sleeplessness faded into oblivion. Thank you for highlighting sleep regularity.
I agree with the good fortune. Hard to know whether good habits lead to luck or luck leads to good habits -- so intertwined.