
The 16-Hour Runway
The most underprescribed intervention in medicine doesn't start at bedtime. It starts the moment you wake up.

Two weeks I wrote about the biology that defends your weight. This week: what it looks like when you change the inputs.
Meet Liam
Liam works on the slope. Two weeks on, two weeks off. On rotation: 6 a.m. to 6 p.m., one hour for lunch. When I first saw him, his day looked like this.
Up at 5:30. Straight to the cafeteria. Eggs, toast, hash browns, coffee. Twelve hours of work with modest walking, about 4,000 steps total. Sedentary lunch in the break room. Off shift at 6, dinner by 6:30. Then TV, phone calls to his wife and kids, internet scrolling, a few snacks taken back to his room. Lights out around 11. Up at 5:30. Repeat for 14 days.
When he came home for his two weeks off, the schedule barely changed. Less walking. No exercise. He enjoyed taking his kids to school but otherwise he meandered through days that looked a lot like his evenings on the slope.
His labs and basic vitals:
Fasting insulin: 17 (early insulin resistance), hba1c 5.8% (pre-diabetes)
Total cholesterol: 220, Triglycerides 220, HDL 37, LDL 142, VLDL 44, Non-HDL 184, Lp(a) 15 nmol/L (reassuringly low)
Blood pressure 139/83, Weight 210 lbs at 5’10” (BMI 30.1)

Every number heading the wrong direction. Not unwell but sliding.
A few years ago I would have started with the following: statin conversation, maybe metformin, dietary counseling. I was not wrong. But now, I focus on the behaviors and habits that set the foundation of health. When I asked Liam how he was sleeping, he paused. Not great. He never feels rested. He has an energy crash every afternoon. Five and a half hours of sleep most nights. His nightlife shows in every line of his lab panel.
I no longer start with Liam’s cholesterol. I start with his day.
5:30 a.m. The Clock Starts
Your body runs two systems that produce sleep. The first is your circadian clock, a 24-hour rhythm governed by the suprachiasmatic nucleus and calibrated primarily by light. The second is sleep pressure: adenosine, a molecule that accumulates in your brain every hour you’re awake. By evening, if you’ve built enough pressure and your circadian clock is properly set, sleep comes. If you haven’t, it doesn’t.
Liam’s first problem was light. On the slope in winter, he walked from his sleeping bunk to the cafeteria and then to the work site in darkness. There is no bright (or natural) light exposure in the first hour of waking. His circadian clock was never properly anchored. A 2025 AHA scientific statement on circadian health now formally recognizes morning bright light as a tool for metabolic regulation: it synchronizes circadian rhythms, promotes daytime alertness and is associated with lower body fat and appetite.
The fix was simple. On clear mornings: 10 to 15 minutes outside before or after breakfast, no sunglasses. On dark mornings: a 10,000-lux light therapy lamp at his desk as soon as he wakes up. The goal isn’t duration of light. It’s timing. Bright light in the first hour anchors the circadian clock that will make sleep possible 16 hours later.
The international expert consensus on indoor light (2022) now uses a metric called melanopic EDI, melanopic equivalent daylight illuminance, as the standard for how light affects the circadian system. The practical translation: most indoor lighting is too dim in the morning and too bright at night. Your office at 300 lux isn’t enough to properly set the clock. Evening scrolling your Iphone at 100 lux in bed is enough to delay it.
6:00 a.m. Breakfast is a Metabolic Decision
Liam’s cafeteria breakfast was carbohydrate-heavy: toast, hash browns, juice and coffee. He was hungry by 9:30 and crashing by 2 p.m. We restructured breakfast around protein.
30+ grams of protein at breakfast. Eggs. We added Greek yogurt or a protein shake on the side. Carbs stayed too, but moved to whole grains and fruit. The fiber target: 30 grams or more across the day. These choices are not about caloric restriction. It is about satiety. Feelin full. Protein and fiber slow gastric emptying, blunt glucose spikes and sustain energy through the morning.
The caffeine conversation. Liam drank coffee at breakfast (fine) and another cup mid-afternoon (not fine). Caffeine’s half-life averages 2.5 to 4.5 hours. A 2023 meta-analysis of 24 studies showed that a single cup of coffee needs about 8.8 hours before bed to avoid measurable reductions in total sleep time. A pre-workout supplement at 200 mg? Closer to 13 hours. These are averages. CYP1A2 polymorphisms, oral contraceptive use and smoking can prolong caffeine’s half-life. Some people are slow metabolizers. A 2 p.m. coffee for a 10 p.m. bedtime was costing Liam sleep he didn’t know he was losing.
We moved his cutoff to one (or two) cup(s) at breakfast. No caffeine after 8 a.m.
12:00 p.m. The Midday Reset
Liam’s lunch was sedentary. Break room, food, phone, back to work. This is where most people miss an opportunity to improve their health.
We made one change: eat first, then walk for 15 to 20 minutes outside (or in the compound). Not a full workout. A walk.
Walking mid-day does three things simultaneously. It builds adenosine (sleep pressure accumulates faster with physical activity than with sitting). It clears the cortisol that’s been building through the morning. It also provides a second dose of bright light that reinforces the circadian signal set at dawn.
Liam added hourly standing breaks during the afternoon: 2 to 5 minutes of movement each hour. Bathroom, water, a short walk. This is NEAT, non-exercise activity thermogenesis. The energy burned through daily movement that isn’t structured exercise. NEAT varies by up to 2,000 calories per day between individuals, doesn’t trigger compensatory hunger and accumulates without requiring willpower or equipment.
For Liam, these small additions moved his daily steps from 4,000 to 8,000 over the first month. No gym required. Organized movement through a day that previously was spent sitting.
4:30 p.m. The Training Window
After his shift, Liam had roughly 90 minutes before dinner. We put a gym session here: 20 minutes cardio, 15 minutes strength. He started at 3 days per week. Eventually this habit turned into a daily routine most days (6/7 on average).
The timing matters. Exercise raises core body temperature. You need that temperature to drop for sleep onset. Training in the late afternoon gives 3 to 5 hours for the body to cool before bed, which is ideal. Training at 9 p.m. can work against the runway we were building.
Strength training wasn’t optional. During any caloric deficit, roughly 25% of weight lost is lean tissue unless you actively maintain it. For a man Liam’s age, 2 to 3 sessions per week with moderate resistance preserves muscle, maintains metabolic rate and supports the glucose disposal that his insulin resistance needed.
6:30 p.m. The Kitchen Closes
Dinner by 6:30. Then the kitchen is closed.
Liam’s old pattern: dinner, then snacks through the evening. Chips, crackers, whatever was in his room. Those calories weren’t feeding hunger. They were feeding boredom and they were wrecking his sleep.
Eating late raises core body temperature at exactly the wrong time. It blunts melatonin onset. It forces the gut into active digestion when the body should be entering recovery mode. A three-hour buffer between the last bite and lights out gives the system time to transition.
This was also where Liam’s evening chronotype was hurting him. The 2026 ADA Standards of Care now recognize evening chronotype as an independent risk factor for type 2 diabetes and is associated with 2.5-fold higher odds of T2DM independent of sleep duration. Liam wasn’t a natural night owl. He’d trained himself into one through a decade of late-night screen time and snacking. Moving dinner earlier and closing the kitchen after was the first step in pulling his sleep time back.
9:00 p.m. The Phone Goes Down
This is the hour most patients resist. Liam’s evenings on the slope were built around his phone: calling his family, watching videos and scrolling news. It was his only connection to home. I wasn’t going to take that away. We reorganized it.
Family calls moved to 7:30, right after dinner. The scrolling, the news, the videos: done by 9. We also moved the phone and his charger to the corner of the room, not the nightstand (as above).
The reason isn’t only blue light, though even ~100 lux of typical indoor lighting can suppress melatonin and delay the circadian clock by up to 1.5 hours. The bigger problem is content. Scrolling activates the sympathetic nervous system. News spikes cortisol. Social media delays sleep onset in ways that aren’t fully explained by light exposure alone.
Liam’s last hour before bed became quiet. He read. He wrote a few notes about the day. Some evenings he just sat. The last hour isn’t empty space. It’s the runway. And what you do in it determines how you land.
We also addressed the room itself. I told Liam what I tell every patient: treat sleep with reverence. The condition, the ritual, the environment. You wouldn’t perform surgery in a noisy room with the lights on. Sleep is a performance too. Room temperature: 64 to 68 degrees. Quiet. Dark. Move the phone across the room, not within arm’s reach.
10:00 p.m. Lights Out
Liam’s old bedtime was 11. His new bedtime: 10. Up at 5:30. That’s 7.5 hours in bed.
This single change, moving bedtime back one hour, may have been the most consequential. Not only is there extra sleep, but the extra hour contains something even more regenerative.
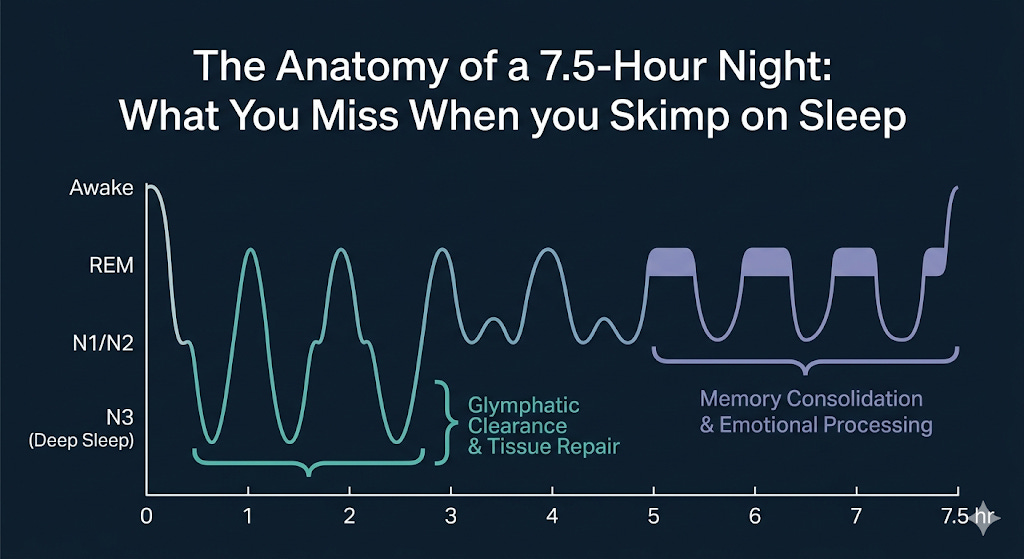
Sleep cycles through stages every ~90 minutes. Deep sleep (N3) concentrates in the first half of the night: this is when the immune system primes, growth hormone releases, tissue repairs and the glymphatic system clears amyloid-beta and tau from the brain. The 2024 AHA scientific statement on sleep and brain health placed glymphatic clearance at the center of dementia prevention. Without adequate deep sleep, the waste products that become Alzheimer’s pathology over decades aren’t cleared.
REM sleep back-loads toward morning: memory consolidation, emotional processing. Go to bed late and you compress the front-loaded deep sleep. Wake too early and you lose the REM cycles you haven’t completed. Liam’s 5.5-hour nights were stealing from both ends.
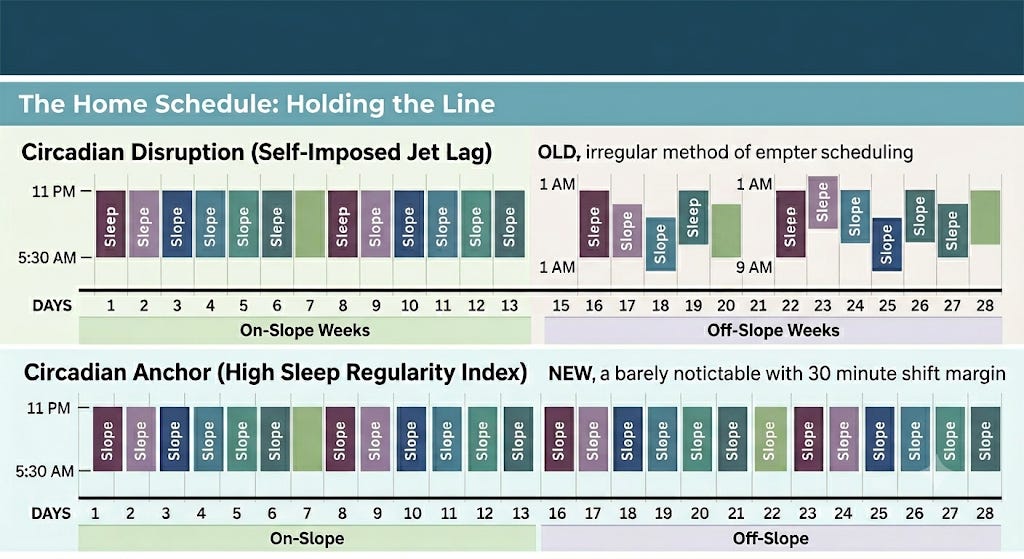
The Home Schedule: Holding the Line
Two weeks off with no externally imposed structure is where most patients lose everything they have built. Liam’s approach at home lost routine: later bedtimes, no movement, no schedule.
Our solution: same architecture, two adjustments.
30 minutes later to bed (10:30, aligned with his spouse)
30 minutes later to rise (6:00)
Same 7.5-hour window. Same circadian rhythm within 30 minutes of the slope schedule.
Morning: kids to school, then walk or gym.
Same meal structure, same protein targets.
Evening: same runway.
The 30-minute shift matters because of what I consider the most important sleep finding of the past five years.
A 2024 UK Biobank study tracked 60,977 people with over 10 million hours of wrist-worn accelerometry. It found that sleep regularity predicted mortality better than sleep duration. People in the most consistent quintile had 20 to 48% lower all-cause mortality compared to the least regular. Adding sleep duration to the model didn’t significantly improve prediction. The 5th percentile of regularity carried a 53% higher mortality risk than the median.
The 2025 AHA scientific statement on multidimensional sleep health now lists regularity as a distinct dimension with independent cardiometabolic implications.
The practical message: going to bed at the same time every night may matter more than how long you sleep. Liam’s two-week rotation had been creating a cycle of circadian disruption every 14 days, a kind of self-imposed jet lag. By keeping his schedule within a 30-minute window between on-slope and off-slope, we eliminated the re-adaptation his biology had been fighting through every month.
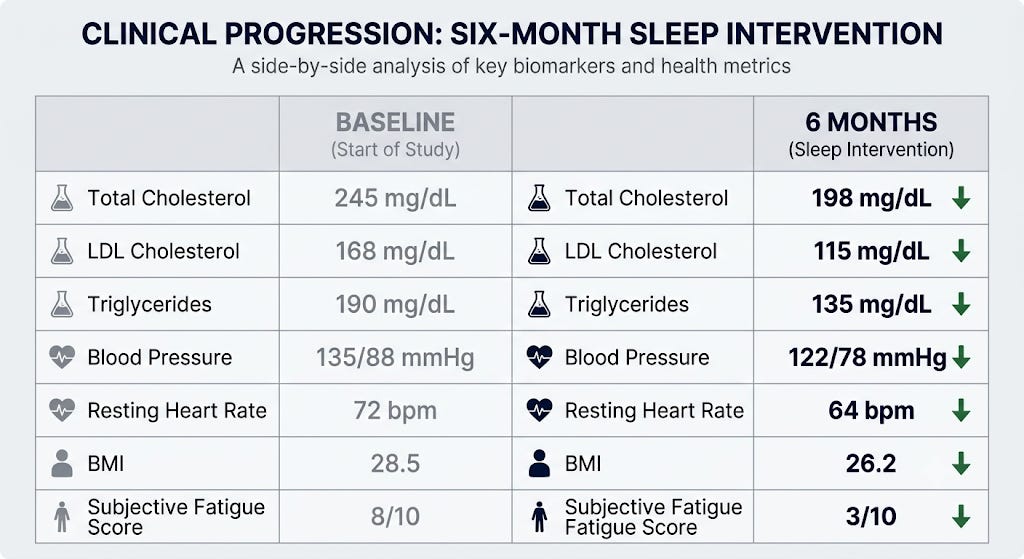
Six Months Later
Liam started tracking with a WHOOP band. Within four weeks: higher sleep efficiency, more time in restorative stages, more consistent overnight heart rate variability. He reported feeling rested for the first time in years. The afternoon crash disappeared.
A note on wearables: a 2025 meta-analysis of 24 validation studies found that consumer wrist-worn devices overestimate total sleep time by about 17 minutes and underestimate wake-after-sleep-onset by about 13 minutes. Sleep/wake detection is reasonably accurate (above 95% sensitivity). Sleep stage classification is not. In head-to-head PSG validation, Oura Ring and WHOOP had the highest multi-state agreement with polysomnography. What to track: weekly average total sleep time, bedtime consistency, resting heart rate trends. What to mostly ignore: night-to-night deep sleep and REM percentages.
Liam tracked what mattered: consistency and duration. Both improved.
His daily steps held at 8,000. His weight moved from 210 to 190. Twenty pounds. A 9.5% reduction.
We repeated labs. Roughly 30% improvement across the board:
Fasting insulin: 17 to 12
HbA1c: 5.8 to 5.4
Triglycerides: 220 to 155
HDL: 37 to 44
LDL: 142 to 118
Non-HDL: 184 to 131
Blood pressure: 139/83 to 124/76
No statin. No metformin. No GLP-1 agonist. A restructured day built around sleep.
The connection between his sleep and his insulin is not speculative. A 2024 randomized crossover trial found that just six weeks of 1.5 hours less sleep per night raised fasting insulin and HOMA-IR without any change in body weight. The 2026 ADA Standards of Care now formally name short sleep as a modifiable risk factor for type 2 diabetes, with up to 50% increased risk at the extremes. Liam’s fasting insulin of 17 wasn’t just about diet. It was about 5.5 hours of sleep, 14 consecutive nights, repeating every month, for years.
His spouse noticed. She adopted a similar schedule. Her sleep improved. She started joining him at the gym on his weeks home. The cascade moved through the household. Well done, Liam.
When the Day Isn’t Enough
Not every patient is Liam. Some patients have optimized the day and still can’t sleep. Two things to rule out.
Chronic insomnia. The first-line treatment is not a sleeping pill. It’s cognitive behavioral therapy for insomnia (CBT-I). A 2024 network meta-analysis confirmed CBT-I produces better long-term remission than pharmacotherapy. About 50% of patients reach remission after 6 to 8 weeks. Digital CBT-I programs (Sleepio, SHUTi, Somryst) now have effect sizes comparable to in-person therapy and outperform medication in head-to-head comparisons. If you’ve been on a sleep medication for years, ask about CBT-I.
Obstructive sleep apnea. If you snore, wake unrefreshed, have a thick neck, or your partner has watched you stop breathing: get evaluated. The STOP-BANG questionnaire is the most sensitive primary care screen. The landscape here changed in 2024: tirzepatide is now FDA-approved for moderate-to-severe OSA in adults with obesity. In the SURMOUNT-OSA trials, it reduced the apnea-hypopnea index by 50 to 59%, and roughly half of patients reached levels where CPAP would no longer be indicated. A 2026 network meta-analysis supports a combined approach: CPAP for airway control, GLP-1 receptor agonists for the underlying metabolic driver. This is a paradigm shift. We’re no longer just treating the airway. We’re treating the disease.
The Prescription
I write sleep prescriptions on a real prescription pad. Every patient gets one (almost).
Rx: Sleep. Dose: 7 to 8 hours. Frequency: Nightly. Refills: Unlimited. Expiration: None.
The data from 2024 through 2026 has made this non-negotiable. Short sleep carries a 14% higher all-cause mortality. Objectively measured sleep under 7 hours raises the risk of heart attack, heart failure, and atrial fibrillation and Mendelian randomization confirms the relationship is causal, not just correlated. Insomnia is associated with a 53% increase in dementia risk. Sleep regularity may predict mortality better than duration.
Sleep is something you work for throughout the day. It is also something that benefits you throughout the day. The work and the reward are the same thing.
Same seriousness as a statin. Larger upside. Cadence is medicine.
If you found this article valuable, share it with someone who is running out of runwayor someone whose health could be transformed by shifting their day.
For individuals who want this integrated approach: where sleep, metabolic architecture and longevity cardiology are treated as a single system visit jakekellymd.com.
Jake Kelly, MD, MHS, FACC is a board-certified performance and preventive cardiologist, ACC Governor for Alaska and founder of ROOL Health, a cardiometabolic longevity practice in Anchorage.
Legal Medical Disclaimer
The information provided on this site including articles, newsletters, social-media posts, videos, and downloadable resources is intended for general educational purposes only and does not constitute medical advice, diagnosis, or treatment. Your use of this content does not establish a physician–patient relationship with me or any contributor. Always seek the guidance of your own physician or another qualified health-care provider before beginning an exercise program, undergoing diagnostic testing, making lifestyle changes, or starting or stopping any medication or supplement. Never disregard professional medical advice or delay seeking care because of something you have read here. If you think you may have a medical emergency, call 911 (or your local emergency service) immediately.
References
American Diabetes Association. (2026). Standards of Care in Diabetes: 2026. Diabetes Care, 49(Suppl 1), S1–S312.
Brown, T. M., Brainard, G. C., Cajochen, C., Czeisler, C. A., Hanifin, J. P., Lockley, S. W. & Wright, K. P. (2022). Recommendations for daytime, evening, and nighttime indoor light exposure. PLoS Biology, 20(3), e3001571.
Cribb, L., Sha, R., Yiallourou, S., Grima, N. A., Cavuoto, M., Baril, A. A., & Pase, M. P. (2023). Sleep regularity and mortality: A prospective analysis in the UK Biobank. eLife, 12, RP89975.
Gardiner, C., Weakley, J., Burke, L. M., Roach, G. D., Sargent, C., Maniar, N., ... & Halson, S. L. (2023). The effect of caffeine on subsequent sleep: A systematic review and meta-analysis. Sleep Medicine Reviews, 69, 101764.
Gottesman, R. F., et al. (2024). Impact of sleep disorders and disturbed sleep on brain health: A scientific statement from the American Heart Association. Stroke, 55(3), e89–e103.
Knutson, K. L., et al. (2025). Role of circadian health in cardiometabolic health and disease risk: A scientific statement from the American Heart Association. Circulation, 151(4), e45–e61.
Malhotra, A., Bednarik, J., Fietze, I., Heinzer, R., Jenkins, M. R., Mansukhani, M. P., ... & SURMOUNT-OSA Investigators. (2024). Tirzepatide for the treatment of obstructive sleep apnea and obesity. New England Journal of Medicine, 391(1), 21–31.
Morin, C. M., & Buysse, D. J. (2024). Management of insomnia. New England Journal of Medicine, 390(12), 1111–1121.
Ungvari, Z., et al. (2025). Imbalanced sleep increases mortality risk by 14-34%: A meta-analysis. GeroScience, 47(3), 4545–4566.
Windred, D. P., Burns, A. C., Lane, J. M., Saxena, R., Rutter, M. K., Cain, S. W., & Phillips, A. J. K. (2024). Sleep regularity is a stronger predictor of mortality risk than sleep duration: A prospective cohort study. Sleep, 47(1), zsad253.
Zuraikat, F. M., Laferrère, B., Cheng, B., Scaccia, S. E., Cui, Z., Aggarwal, B., Jelic, S., & St-Onge, M. P. (2024). Chronic insufficient sleep in women impairs insulin sensitivity independent of adiposity changes: Results of a randomized trial. Diabetes Care, 47(1), 117–125.
Lots of great information here. I am a board certified wellness coach and health navigation coach and this information directly addresses what I coach on. Thank you for the work you are doing. Great read!
Great information! Having previously worked night shifts in a hospital and day shifts on the slope as an RN I’ve lived the struggle of not getting enough sleep. Kudos to Liam for instituting your suggestions!