
Under Pressure
What one patient taught me about treating the person, not just the number.

John was referred to me for refractory hypertension. He was 62. Already on three medications: amlodipine 10 mg, hydrochlorothiazide 25 mg and losartan 100 mg. In the clinic, his blood pressure was 162/97.
John was larger than life. Six foot five, 243 pounds. He is very active remodeling his home by hand. He doesn’t sit around worrying about his health. But over the prior two years, his primary care physician had watched his BP climb. He started one medication. Then another. And another. His BP kept rising. Then a referral came to me.
We discussed the DASH diet, the importance of building a foundation of healthy food choices, sleep patterns and physical activity. John wasn’t excited about taking more pills. His potassium was low-normal. He didn’t want to change the medications he was already on. So we added a fourth, spironolactone, a mineralocorticoid receptor antagonist starting at 25 mg.
Three days later, he called my nurse. His blood pressure was worse.
I increased the spironolactone to 50 mg. John was dutiful. He took the higher dose. His blood pressure climbed further: 173/103 on his home cuff.
Four medications. Higher numbers.
I did not know what to do next.
I’ll come back to John. But his clinical response suggested I was planting weeds in his garden. I was focused on reducing a number without treating the person. More medications was not the answer. Understanding what was actually driving up his pressure was the needed solution.
I had to shift my thinking in how I approach hypertension.
For a deeper look at the cardiovascular prevention framework I use with patients, see my previous article on fitness, circulation and metabolism.
The 2025 Guidelines: What Actually Changed
The AHA/ACC released updated hypertension guidelines in 2025, which was the first major revision since 2017, when hypertension was redefined as 130/80 mmHg.
The categories haven’t changed:
Normal: Less than 120/80 mmHg
Elevated: Systolic 120–129 and diastolic less than 80
Stage 1 Hypertension: Systolic 130–139 or diastolic 80–89
Stage 2 Hypertension: Systolic 140+ or diastolic 90+

The changes are reflected in how we act on these numbers.
The 2025 guidelines recommend that low-risk adults with stage 1 hypertension (130–139/80–89) who don’t improve after three to six months of lifestyle modification should start medication: targeting below 130/80. Previously, these patients were told to “watch and wait.”
The old Pooled Cohort Equations are retired. The PREVENT risk calculator replaces them, incorporating kidney function, statin use and social determinants of health. This is a more nuanced tool to help decide who needs treatment and how aggressively.
The universal target: less than 130/80 mmHg for all adults, with individualized exceptions for institutionalized patients, limited life expectancy and pregnancy.
The threshold for concern moved earlier, while the threshold for action moved with it.
How to Check Blood Pressure
Blood pressure measurement sounds simple. It isn’t. Most people measure it wrong.
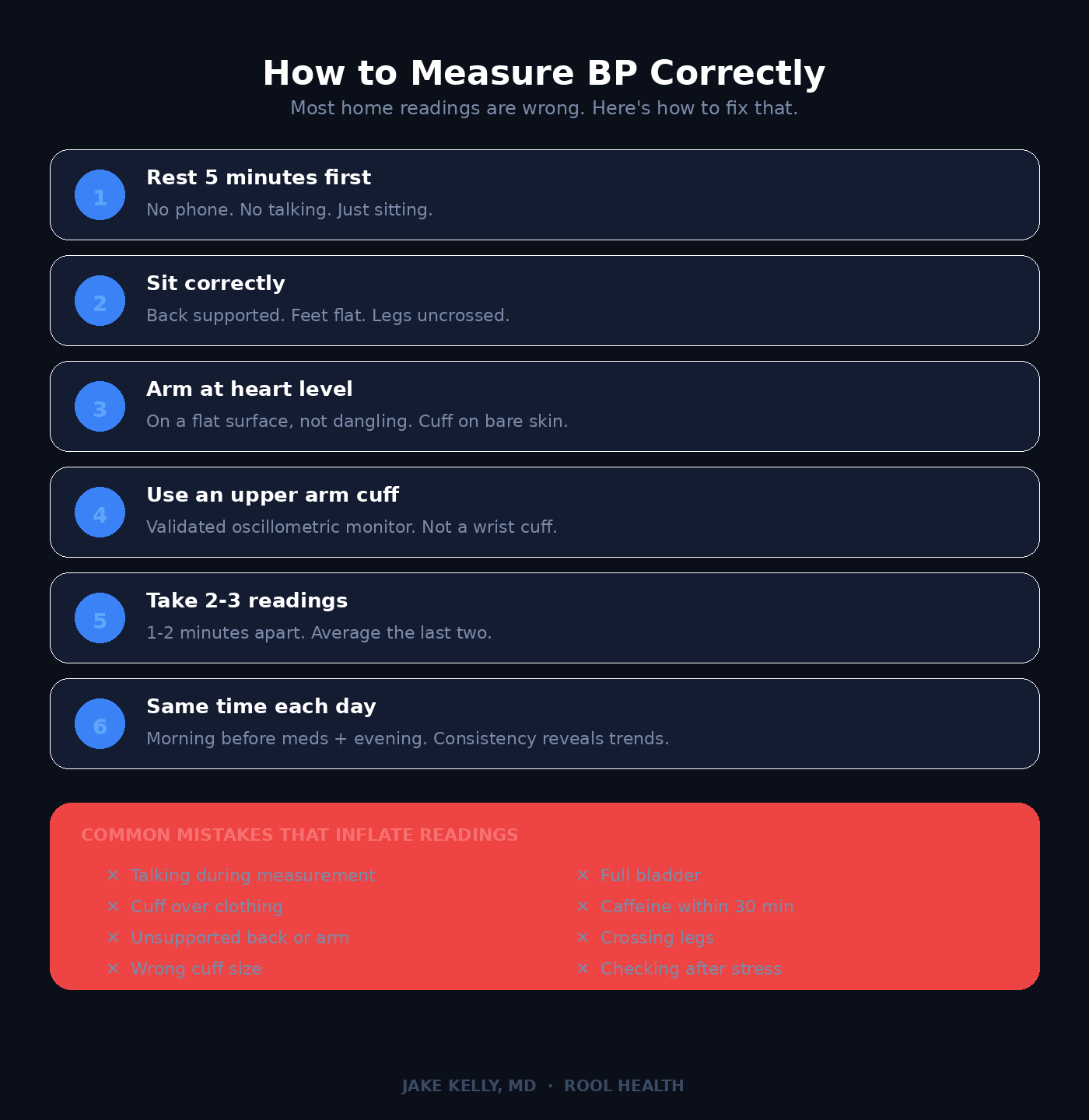
Body position, arm support, cuff size, time of day, caffeine, bladder fullness, talking during the measurement; there are dozens of variables that affect BP accuracy. Most BP readings people take at home are inaccurate. Many BPs taken in clinic offices are too.
The Right Way to Check BP
Sit quietly for five minutes before measuring. Don’t scroll on your phone. Do not talk. Sit still. Keep your feet flat on the floor. Support your back. Rest your arm at heart level on a flat surface. Do not dangle your arm at your side. Place the cuff on bare skin, not over clothing.
Take two to three BP readings, one to two minutes apart. Average the last two.
When to Check
Blood pressure follows a circadian rhythm. It’s lowest during sleep, rises sharply in the early morning hours and tends to peak in the late afternoon or early evening. For most people, the best time to check their BP is in the morning before medications and again in the evening… at the same times each day (for comparison).
How Often
This depends on where you are:
Known hypertension or on medication: a few times per week. Daily during medication adjustments, then periodic once stable.
Elevated but untreated hypertension: two to three times per week gives a reasonable picture of your trajectory.
Healthy with normal readings: at least annually. Over 40 or with risk factors including family history, obesity, diabetes and kidney disease: quarterly or biannually.
The point isn’t obsessive measurement. It’s establishing a pattern. One reading means little. A trend over weeks tells you something real.
Office vs. Home: Which One Matters More?
Both BP readings yield insight but they tell you different things.
Office readings are often higher than home readings: this is a phenomenon called the “white coat effect.” Some people have the reverse: normal in the office, elevated at home. This is called masked hypertension and it’s arguably more dangerous because it goes undetected.
Home blood pressure monitoring (HBPM) gives you the volume of data that a clinic visit never can. It’s now a cornerstone of the 2025 guidelines for confirming diagnoses and titrating treatment.
Ambulatory Blood Pressure Monitoring (ABPM)
For certain patients, 24-hour ambulatory blood pressure monitoring is the gold standard. You wear a cuff that inflates automatically every 15 to 30 minutes throughout the day and night.
ABPM is particularly useful for detecting white coat hypertension, masked hypertension, nocturnal non-dipping (blood pressure that doesn’t fall during sleep which is a strong independent risk factor), suspected episodic hypertension and resistant hypertension that isn’t responding to treatment. If your office readings and home readings don’t match, or if your hypertension seems resistant to medications, ABPM can clarify what’s actually happening.
The Right Device
Use an upper arm cuff with an oscillometric monitor. Not a wrist cuff. Wrist devices are less reliable due to positioning variability and tend to overestimate or underestimate true brachial artery pressure.
Make sure your cuff is validated. The AMA’s website (validatebp.org) maintains a list of validated monitors. If your home device consistently reads 5+ mmHg differently from your physician’s office, bring it in for a side-by-side comparison. That’s how you calibrate.
The Dentist Connection
Your dentist may be the one who catches your high blood pressure.
The ADA now recommends routine blood pressure screening at dental visits. Many adults see their dentist more regularly than their physician: this is an underutilized screening opportunity.
Dental offices typically use wrist cuffs, which are less accurate, especially if the wrist isn’t at heart level. If a wrist reading comes back elevated, follow up with a validated upper arm measurement. A dental BP check is a signal, not a diagnosis.
The ADA recommends deferring elective treatment for readings above 160/100 and urgent medical referral above 180/110. Another reason your dentist should be part of your prevention team.
What Actually Drives High Blood Pressure
This is where John’s case pushed me deeper.
We treat blood pressure as a hemodynamic problem. Too much pressure: add a vasodilator. Too much volume: add a diuretic. Hypertension is rarely that simple.
Blood pressure is the downstream expression of converging systems: sympathetic activation, the renin-angiotensin-aldosterone axis, endothelial function, arterial stiffness, insulin resistance, sleep architecture, visceral adiposity and chronic stress. When we only intervene at the drug level, we treat the output without addressing the inputs.
Two under-diagnosed drivers of hypertension deserve specific mention. Primary aldosteronism, once considered rare, is now estimated in 5 to 25 percent of hypertensive patients. The 2025 guidelines expanded screening to all patients with stage 2 or resistant hypertension. It’s still massively under-diagnosed. Obstructive sleep apnea is even more common: present in 25 to 50 percent of hypertensive patients. Fragmented sleep drives sustained sympathetic activation and no amount of medication fully compensates for a disordered airway eight hours a night. If your blood pressure isn’t responding to treatment, these two diagnoses should be actively excluded.
Medications move the needle. But they work best when the foundation is solid: when sleep is restored, the body is moving, the stress response isn’t running 16 hours a day and the diet isn’t silently working against every pill.
John taught me to ask a different question. One should not ask “which drug should I add?” We should inquire, “what is driving this pressure up?”
Lowering Blood Pressure Naturally: What the Evidence Actually Shows
For stage 1 hypertension, stacking multiple lifestyle changes can rival a single medication. For stage 2, lifestyle alone is rarely sufficient, but it remains foundational, even when drugs are added.
Here’s what the data supports.
Diet: The DASH Framework
The DASH diet (Dietary Approaches to Stop Hypertension) remains the most evidence-backed dietary intervention for blood pressure: fruits, vegetables, whole grains, lean proteins, low-fat dairy, limited sodium and saturated fat.
The effect sizes are real. DASH alone: 5 to 7 mmHg systolic reduction. Combined with sodium restriction below 2,300 mg/day (ideally 1,500 mg): reductions exceeding 11 mmHg systolic in hypertensive individuals. This is comparable to many first-line medications.
Sodium and potassium intake are relevant. The ratio between the two may be more important than absolute sodium intake. A diet rich in potassium (bananas, spinach, sweet potatoes, avocados) helps counterbalance sodium’s pressor effects through enhanced renal sodium excretion and direct vascular relaxation.
Alcohol reduction warrants mention (less so for our Generation Z population who imbibe minimally). Chronic alcohol consumption above two drinks per day is independently associated with hypertension. Reducing intake to one drink or less per day can lower systolic BP by 2 to 4 mmHg, which is a modest but additive effect when stacked with other interventions.
Aerobic Exercise
150 minutes per week of moderate intensity (or 75 minutes of vigorous activity) lead to approximately 5 to 8 mmHg systolic reduction. Exercise’s mechanism works through improved endothelial function, reduced sympathetic tone and favorable vascular remodeling.
The key word is consistent. A single session’s effect lasts 12 to 24 hours (post-exercise hypotension). Stop exercising, the effect vanishes within weeks. This is not a treatment you earn and keep. It’s a practice you maintain.
Walking counts. Swimming. Cycling. Zone 2 training: where you can hold a conversation (2-3 sentences without taking a deeper breath) but not sing builds the aerobic base. For blood pressure specifically, steady moderate-intensity exercise five days a week is the most supported protocol.
10-minute physical activity bouts accumulated through the day confer measurable benefit. The barrier to entry is low. The physiologic return is high.
Resistance Training
Traditionally, resistance training was viewed with caution in hypertensive patients; the concern being acute spikes during heavy lifts. The evidence has evolved.
Regular dynamic resistance training (weightlifting, machines, bodyweight exercises) reduces resting blood pressure modestly: roughly 2 to 5 mmHg systolic. It’s not as potent as aerobic training for BP reduction, but its contributions to metabolic health, body composition and functional capacity make it indispensable.
Isometric Exercise: The Emerging Standout
This is the data point that surprises most people.
A 2023 network meta-analysis in the British Journal of Sports Medicine ranked isometric exercise (wall sits isometric handgrip) as the single most effective exercise modality for reducing resting blood pressure. More effective than aerobic. More effective than resistance training or HIIT.
The numbers: ~8 mmHg systolic and 4 mmHg diastolic. A 2025 multilevel meta-review confirmed it: 8.2/4.0 mmHg reductions.
The protocol is simple: four sets of two-minute holds with one to four minutes rest, three times per week. I recommended starting at 30 second holds and building by 30 seconds each session as you build strength, focus and resilience. Less than 30 minutes a week.
Isometric exercises do not replace aerobic or resistance training. It complements them. But for patients who are deconditioned, time-limited or looking for an additional lever, isometric holds are legitimate and evidence-backed.
Tai Chi
Approximately 6/3 mmHg reduction, with effects strengthening after 12 weeks of consistent practice. A 2024 RCT in JAMA Network Open found Tai Chi matched conventional aerobic exercise for blood pressure reduction in prehypertension.
Low-intensity movement, controlled breathing and sympathetic modulation. For older adults or those who can’t tolerate traditional exercise, Tai Chi is a credible, meaningful addition.
Mindfulness and Stress Reduction
Chronic stress elevates blood pressure through sustained sympathetic activation and cortisol-driven sodium retention. Mindfulness-based stress reduction programs: roughly 2 to 5 mmHg systolic in meta-analyses.
Smaller than diet or exercise. But for patients with high stress loads, it addresses a mechanism medications don’t directly target.
Weight Loss
Every kilogram lost leads to approximately 1 mmHg systolic reduction. A 5 kg loss: ~4.4/3.6 mmHg.
For patients carrying excess visceral fat, where insulin resistance, sympathetic overdrive and aldosterone excess converge, weight loss attacks root physiology. Sometimes it’s the single most impactful intervention.
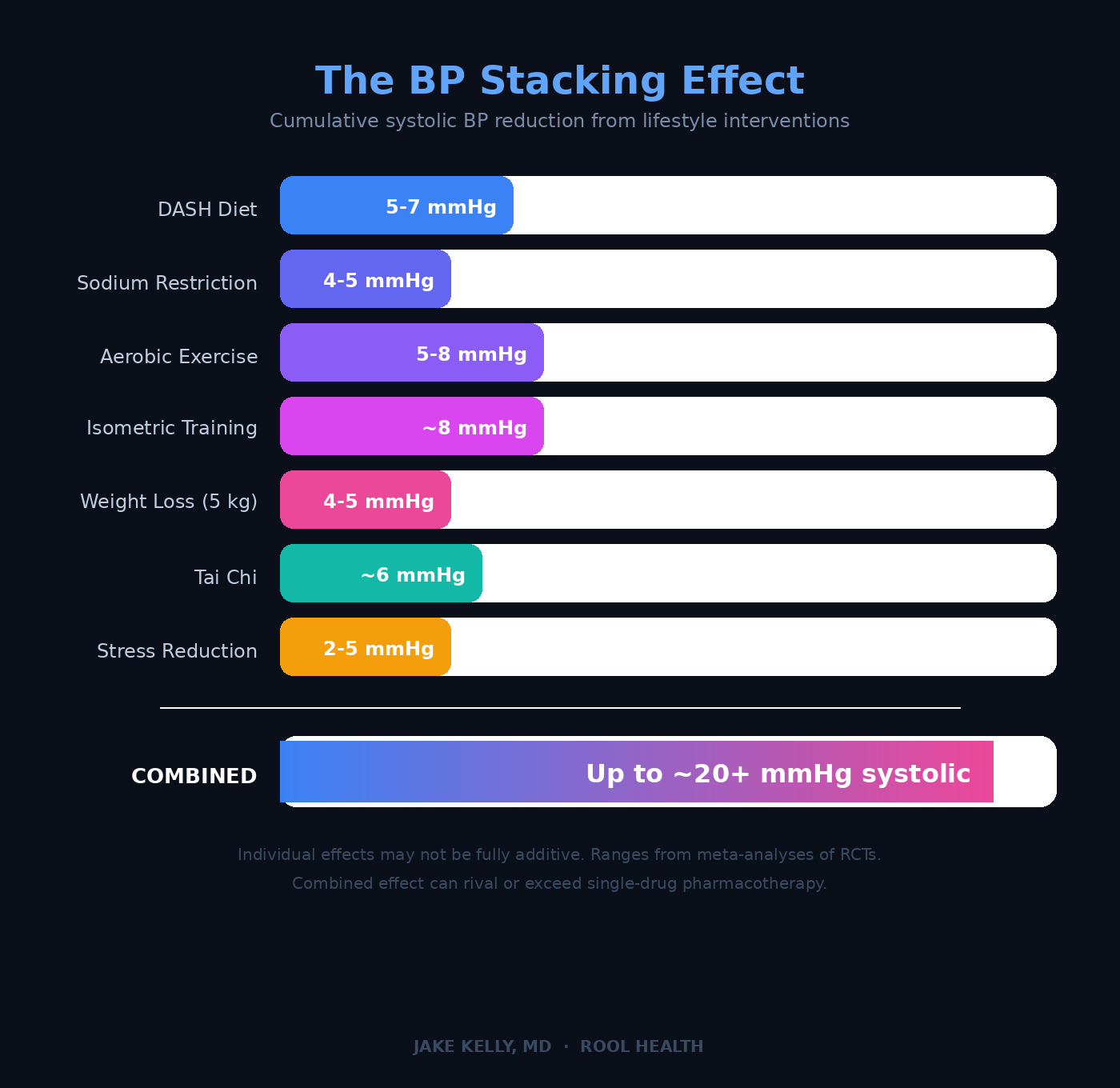
The Stacking Effect
No single lifestyle change matches the efficacy of combination pharmacotherapy. Stack them together: DASH diet with sodium restriction, regular aerobic exercise, isometric training, weight loss and stress management. Now you’re looking at cumulative reductions that can approach 20 mmHg systolic or more.
That’s meaningful. This behavior modifications will change your BP and health trajectory.
Back to John
With four medications failing, I did what I should have done earlier. I stepped back.
We performed a full secondary hypertension workup: renin-aldosterone ratio, renal artery ultrasound, sleep apnea testing and plasma metanephrines. No pheochromocytoma. No renal artery stenosis. No primary aldosteronism. The usual suspects were cleared.
So I looked at John’s life.
Remodeling his home: essentially a second full-time job. The physical activity was there, but the stress was relentless. Sleep was fragmented. His diet wasn’t terrible: low salt but it wasn’t structured. At 243 pounds on a 6’5” frame, BMI didn’t flag him. But he was carrying more visceral weight than the number suggested.
We built a different plan. Structured stress management, not “try to relax.” Tai Chi. Bodyweight exercises including isometric holds. Weight consciousness, no crash diet. Deliberate attention to what he was eating. Good sleep hygiene.
We simplified his medications. We stopped chasing the number with more drugs. Focus on the right drugs at the right doses for his physiology.
John went from four medications to two: hydrochlorothiazide 25 mg and losartan 50 mg. Lower doses. Better blood pressure.
One patient taught me ten years of hypertension management.

I write about cardiovascular prevention; the signals that matter before symptoms show up. If that’s useful to you, subscribe.
When an Isolated High Reading Isn’t an Emergency and When It Is
You check your blood pressure at home. It reads 165/95. Should you go to the ER?
Probably not.
An isolated elevated reading without symptoms is common. Anxiety, caffeine, a full bladder, a recent argument: dozens of things cause transient spikes. Sit. Rest five minutes. Recheck.
The framework:
Below 180/120 with no symptoms: Recheck. If consistently elevated, contact your physician for follow-up. Not an emergency.
180/120 or higher without symptoms (hypertensive urgency): Contact your doctor the same day. This usually doesn’t require hospitalization, but it does require prompt evaluation and likely medication adjustment.
180/120 or higher with symptoms…chest pain, shortness of breath, severe headache, vision changes, numbness, back pain or difficulty speaking (hypertensive emergency): Call 911. This is end-organ damage in progress. Minutes matter.
The distinction between urgency and emergency is the presence of target organ injury. The number alone doesn’t tell you enough. Context matters.

Medications: The Four Drug Classes You Need to Understand
When lifestyle isn’t sufficient or when blood pressure warrants immediate treatment, medications become necessary. John’s story doesn’t mean medications are the enemy. It means they work best when the foundation is solid.
Four first-line classes, each targeting a different mechanism:
1. ACE Inhibitors (lisinopril, enalapril, ramipril)
Block the conversion of angiotensin I to angiotensin II, reducing vasoconstriction and aldosterone secretion. Well-studied for renal protection in diabetes and heart failure. Main side effect: a persistent dry cough in roughly 10 to 15 percent of patients, driven by bradykinin accumulation.
2. Angiotensin Receptor Blockers or ARBs (losartan, valsartan, telmisartan)
Block angiotensin II at the receptor level. Similar efficacy to ACE inhibitors without the cough. The LIFE trial demonstrated that losartan reduced cardiovascular morbidity and mortality more than atenolol for a similar degree of blood pressure reduction suggesting benefits beyond hemodynamics alone, including regression of left ventricular hypertrophy.
3. Calcium Channel Blockers (amlodipine, nifedipine)
Reduce calcium influx into vascular smooth muscle cells, promoting vasodilation. Effective across a broad range of patients. The ALLHAT trial, one of the largest antihypertensive trials ever conducted, showed that amlodipine was non-inferior to chlorthalidone for preventing fatal coronary heart disease and nonfatal MI.
4. Thiazide Diuretics (chlorthalidone, hydrochlorothiazide, indapamide)
Reduce blood volume through sodium excretion. ALLHAT established chlorthalidone as a reference standard: it was at least as effective as the newer agents for major cardiovascular outcomes and less expensive. The guidelines still recommend thiazide-type diuretics as a strong first-line option, particularly when cost is a consideration.
The ALLHAT Legacy
ALLHAT (Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial) fundamentally shaped how we prescribe. Over 33,000 high-risk patients. Newer, more expensive drugs didn’t outperform thiazide diuretics for hard cardiovascular endpoints. Evidence should guide prescribing…not marketing.
Combination Therapy and Single-Pill Combinations
The 2025 guidelines favor early combination therapy. Use two agents simultaneously rather than sequentially titrating one drug. Two drugs at lower doses often achieve better reduction with fewer side effects than one drug at max dose.
Single-pill combinations improve adherence and are now a Class I recommendation. An ACE inhibitor or ARB paired with a calcium channel blocker or thiazide is a common, well-tolerated start.
For resistant hypertension, blood pressure that remains above target despite three drugs including a diuretic, spironolactone (a mineralocorticoid receptor antagonist) is the recommended fourth-line agent. In the PATHWAY-2 trial, it proved superior to other add-on agents for resistant hypertension.
For patients who remain uncontrolled despite optimal medical therapy, renal denervation, a catheter-based procedure that disrupts sympathetic nerve signaling to the kidneys, is now included in the 2025 guidelines for the first time. It’s not first-line. It’s not for everyone. But for select patients with resistant hypertension and preserved kidney function (eGFR ≥40), it’s a real option guided by a multidisciplinary team.
What’s on the Horizon
The next wave of antihypertensives targets mechanisms we’ve never been able to reach with existing drugs.
Baxdrostat, an aldosterone synthase inhibitor, showed placebo-adjusted systolic reductions of ~9 to 10 mmHg in the BaxHTN trial for resistant hypertension. It blocks aldosterone production at its source, upstream of spironolactone’s mechanism, without the anti-androgen side effects.
Zilebesiran uses RNA interference to silence hepatic angiotensinogen synthesis. One subcutaneous injection every six months.
Aprocitentan, an endothelin receptor antagonist, is FDA-approved for resistant hypertension.
These emerging therapies are not replacements for the foundational four drug classes. For the subset of patients with truly resistant hypertension, the therapeutic landscape is expanding in ways we haven’t seen in decades.
How Low Is Too Low?
This is a question I get often. Patients can feel dizzy or fatigued on their medications.
For most healthy adults, a systolic blood pressure in the 90s is not inherently dangerous, provided you feel well. Many endurance athletes live comfortably at 90/50.
Context changes the calculus.
Heart failure with reduced ejection fraction (HFrEF): These patients are often on multiple BP-lowering agents: ACE inhibitors or ARBs, beta-blockers, sacubitril-valsartan, spironolactone. Each therapy is guideline-directed. Improves survival. The cumulative effect on blood pressure can be substantial. I’m often navigating a narrow corridor, low enough for cardiac remodeling, high enough to avoid symptomatic hypotension and kidney injury. Systolic pressures of 80 to 90 are common and sometimes acceptable, but they require close monitoring.
Spironolactone for non-cardiac indications: Increasingly prescribed for acne, hormonal hair loss, and PCOS. It’s a potassium-sparing diuretic with real BP-lowering effects, especially above 50 mg. Only about 3 percent of women on it for acne experience absolute hypotension but the risk rises if you’re already on antihypertensives or have low baseline pressures. If you’re on spironolactone for any reason, check your blood pressure.
Older adults and orthostatic hypotension: Standing blood pressure should be checked in any elderly patient on antihypertensives. A drop of more than 20 mmHg systolic upon standing is orthostatic hypotension. This is a fall risk.
If You’re Healthy, How Often Should You Check?
Consistently normal, no medications, no risk factors: annual screening is sufficient for most people under 40.
After 40, or with risk factors of family history, obesity, sedentary lifestyle, twice a year.
For the health-conscious individual who wants to stay ahead of drift: once a quarter. Because blood pressure drifts upward with age. Arterial stiffness increases. Sodium sensitivity shifts. What was 115/72 at 35 becomes 128/78 at 50 without any obvious lifestyle change.
The goal isn’t to catch a crisis. It’s to detect the trajectory before it becomes a diagnosis.
The Bigger Picture
John didn’t need more pressure from his medications. He needed less pressure in his life.
This distinction, treating a number versus treating a person, is the difference between reactive medicine and performance-driven prevention.
Blood pressure isn’t just a reading on a cuff. It’s a window into vascular health, autonomic balance, metabolic function, and the cumulative stress load of a life.
Measure consistently. Intervene early. Add medication when physiology demands it. Track the trajectory over years.
The 2025 guidelines reinforce what we’ve known but too often ignored. Earlier detection, earlier action, lower targets for everyone.
Measure what matters. Build the reserve.
—Jake
Legal Medical Disclaimer
The information provided on this site including articles, newsletters, social-media posts, videos, and downloadable resources is intended for general educational purposes only and does not constitute medical advice, diagnosis, or treatment.
Your use of this content does not establish a physician–patient relationship with me or any contributor. Always seek the guidance of your own physician or another qualified health-care provider before beginning an exercise program, undergoing diagnostic testing, making lifestyle changes, or starting or stopping any medication or supplement.
Never disregard professional medical advice or delay seeking care because of something you have read here. If you think you may have a medical emergency, call 911 (or your local emergency service) immediately.
References
Jones DW, et al, et al. 2025 AHA/ACC Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults. Hypertension. 2025.
ALLHAT Officers and Coordinators. Major outcomes in high-risk hypertensive patients randomized to ACE inhibitor or calcium channel blocker vs diuretic. JAMA. 2002;288(23):2981-2997.
Dahlof B, et al. Cardiovascular morbidity and mortality in the Losartan Intervention For Endpoint reduction in hypertension study (LIFE). Lancet. 2002;359(9311):995-1003.
Edwards JJ, et al. Exercise training and resting blood pressure: a large-scale pairwise and network meta-analysis of randomised controlled trials. Br J Sports Med. 2023;57(20):1317-1326.
Sacks FM, et al. Effects on blood pressure of reduced dietary sodium and the DASH diet. N Engl J Med. 2001;344:3-10.
Neter JE, et al. Influence of weight reduction on blood pressure: a meta-analysis of randomized controlled trials. Hypertension. 2003;42(5):878-884.
Zhong D, et al. Effect of Tai Chi vs Aerobic Exercise on Blood Pressure in Patients With Prehypertension: A Randomized Clinical Trial. JAMA Network Open. 2024.
Williams B, et al. Spironolactone versus placebo, bisoprolol, and doxazosin to determine the optimal treatment for drug-resistant hypertension (PATHWAY-2). Lancet. 2015;386(10008):2059-2068.
American Dental Association. Hypertension Screening Guidelines. ada.org.
You and your family have a wonderful Easter.
Another medical ‘clinic’ for the public and professionals. The time commitment required to issue essays of this depth and caliber makes me wonder when you squeeze in a patient or two. Well done, Jake!